Content warning Portions of descriptions and imagery on this page contain inaccurate views, derogatory language, and offensive imagery. They are included here as they were originally created in order to compile a complete reproduction. They do not reflect the attitudes of this site’s creator.
![]() General Considerations
General Considerations
 General Considerations
General ConsiderationsPosition of Man in Organic Nature.
Linnæus placed man at the head of the animal kingdom, presenting what he deemed his most important characteristic, in the specific name Sapiens.
Other naturalists have expressed themselves quite indignantly against even this approximation to the brute creation, denying the propriety of grouping man with other Mammalia. Nevertheless, it is impossible to deny that in many respects there is a close resemblance to the higher quadrumana in many external features, and a still more intimate relation in the fundamental points of anatomical and physiological structure. By placing him; in the order Bimana, of which he is sole occupant, we make a zoological difference from the monkeys and apes, this difference being vastly increased by the presence of intelligence and reason.
However great the resemblance between Man and the Quadrumana, yet the differences, as already remarked, are sufficient to prevent their ever being approximated more closely than we have done. Thus, a perfectly opposable thumb is unknown among the monkey tribe; this member, although, capable of grasping objects, is yet unable to act with the delicacy and precision so eminently characteristic in man. The erect attitude, too, is man’s sole prerogative; this involving numerous differences in general structure. Another point of difference is to be found in the different facial angle; this being such as to throw the face immediately beneath the brain, and not anterior to it. This facial angle is formed by two ideal lines, one drawn from the most projecting portion of the forehead to the anterior extremity of the alveolar margin of the upper jaw, the other extending from the latter point in a horizontal direction through the meatus auditorius externus. The development of brain will generally be found to bear a certain ratio to the obtuseness of this angle. Pl. 119, fig. 10, exhibits the facial angle of the European; fig. 11, that of the negro; and fig. 12, that of the orang-outang.
Other important characteristics of mankind are to be found in the absence of any intervals between contiguous teeth, and in the vertical position of the latter; in the comparatively small size of the face, the prominent chin, the broad foot, the long muscular legs; in his capacity of having under great extremes of heat and cold; his adaptation to a purely animal or vegetable diet, as well as to a mixture of the two, &c. But by far the most important characters are to be found in those mental endowments which distinguish him so eminently from the brute.
Varieties of Mankind

Glossary for plate 119
- I. Kaukasische oder Weisse Race, Caucasian or White Race.
- II. Mongolische oder Gelbe Race, Mongolian or Yellow Race.
- III. Æthlopische oder Schwarze Race, Ethiopian or Black Race.
- IV. Armerikanische oder Kupferfarhige Race, American or Copper-colored Race.
- V. Malayische oder Olreenfarhige Race, Malay or Olive-colored Race.
- F. 1 bis 4. Grundzüge (Typus) der Kaukofischeri Race, Figs. 1–4. Types of the Caucasian Race.
- Figur 5. Grundzüge der Mongolischen Race, Fig. 5. Type of the Mongolian Race.
- Figur 6. Grundzüge der Æthiopischen Race, Fig. 6. Type of the Ethiopian Race.
- F. 7, 8. Grundzüge der Kupferfarbigen Race, Figs. 7, 8. Type of the Copper-colored Race.
- Figur 9. Grundzüge der Olivenfarbigen Race, Fig. 9. Type of the Olive-colored Race.
- Afghanen, Afghans.
- Algonkiren, Algonkins.
- Araber, Arabs.
- Azteken, Azteks.
- Berbern, Berbers.
- Birmanen, Birmans.
- Bucharen, Bucharians.
- Caffern, Caffres.
- Californier, Californians.
- Canadier, Canadians.
- Caraiben, Caribbeans.
- Celten, Celts.
- Chaldäer, Chaldseans.
- Chinesen. Chinese.
- Cinbebassen, Cinbebasses.
- Colombier, Colombians.
- Eleuten, Aleutians.
- Eskimos, Esquimaux.
- Ethiopier, Ethiopiana.
- Fellatas, Fellatah.
- Finnen, Finns.
- Germanen, Germans.
- Gothen, Goths.
- Hindus, Hindoos.
- Hottentotten, Hottentots.
- Iberier, Iberians.
- Jakuten, Yacoots.
- Japanesen, Japanese.
- Jukaghiren, Youkaghii’S.
- Kalmückcn, Calmucks.
- Kamtsckadalen, Kamskadales.
- Kaukasier, Caucasians.
- Kirghisen, Kirghese.
- Koriälen, Koreans.
- Kosaken, Cossacks.
- Kriks, Creek Indians.
- Lappen, Laplanders.
- Letten, Lethonians.
- Madagassen, Madagassees.
- Mandschus, Manchoos.
- Mauren, Moors.
- Mongolen, Mongols.
- Neger, Negroes.
- Negritos, Negritoes.
- Neuseeländer, New Zealanders.
- Osagen, Osages.
- Osmanen, Osmanli.
- Ostiaken, Ostiaks.
- Patagonen, Patagonians.
- Pelasger, Pelasgians.
- Perser, Persians.
- Samojeden, Samoeids.
- Sius, Sioux Indians.
- Slaven, Slavonians.
- Soyten, Soyetes.
- Tibetaner, Thibetans.
- Tschucktschen, Tchoukches.
- Tungusen, Tungus.
- Wogulen, Voguls.
It is not our purpose to enter upon the question now agitating the scientific world, as to whether mankind be descended from one pair or from several; and if the latter, whether these original pairs were of one single species, or of a greater number. The problem is still far from being solved, requiring the combined efforts of the anatomist, the physiologist, the zoologist, the philologist, and the theologian. Nowhere is a severe application of all the principles of modern scientific investigation more necessary to a satisfactory conclusion than in this instance.
Any attempt at a systematic classification of man, as at present distributed over the surface of the globe, is attended with great difficulties. Although in typical individuals of different nations strongly marked features of distinction may be observed, yet, when we attempt to include mankind in one general arrangement, we find such an endless variety, such insensible gradations from one form into another, such unexpected anomalies in particular circumstances, as almost to cause the ethnologist to throw down his pen in despair. It is for this reason that different authors have had such apparently contradictory views as to the number of principal races, and their proper sub-divisions. Thus, Desmoulins gives sixteen such races; Bory de St. Yincent, fifteen; Prichard, seven; Blumenbach, five; while Cuvier makes only three. The five races of Blumenbach are termed by him:—Caucasian, Mongolian, Ethiopian, Malay, and American. Cuvier refers the Malay race to the Ethiopian, and the American to the Mongolian, leaving only the Caucasian, Mongolian, and Ethiopian.
Dr. Chas. Pickering, in his important work entitled “The Faces of Man,” gives eleven races, as follows:
- White.
- Arabian. Nose prominent; lips thin; beard abundant; hair straight and flowing.
- Abyssinian. Complexion hardly becoming florid; nose prominent; hair crisped.
- Brown.
- Mongolian. Beardless; with the hair perfectly straight, and very long.
- Hottentot. Negro features, and close woolly hair; stature diminutive.
- Malay. Features not prominent in the profile; complexion darker than in, the preceding races; the hair straight, or flowing.
- Blackish-brown.
- Papuan. Features not prominent in the profile; beard abundant; skin harsh to the touch; hair crisped or frizzled.
- Negrillo. Apparently beardless; stature diminutive; features approaching those of the negro; hair woolly.
- Indian or Telingan. Features approaching those of the Arabian; the hair in like manner straight or flowing.
- Ethiopian. Complexion and features intermediate between those of the telingan and negro; hair crisped.
- Black.
- Australian. Negro features, combined with straight or flowing hair.
- Negro. Close woolly hair; nose much flattened; lips very thick.
In the present brief reference to the principal subdivisions of the human race, we shall follow Latham, who, in his recent work entitled “Natural History of the Varieties of Man,” has treated of the subject in a highly scientific manner, and has given to it as much precision as perhaps it is capable of at the present time.
The following table exhibits the principal divisions and subdivisions employed by Mr. Latham, and we shall take up their consideration in the same order:
-
Mongolidæ.{
-
Altaic.{
-
- Seriform.
- Turanian.
-
- Dioscurian.
-
Oceanic.{
-
- Amphinesian.
- Kelænonesian.
-
- Hyperborean.
- Peninsular.
- American.
- Indian.
-
-
Atlantidæ.{
- Negro. Western, Central, Eastern.
- Caffre. Western, Central, Eastern.
- Hottentot. Hottentot, Saab.
- Nilotic. Gallahs, Agows, Nubians, Bisharis.
- Amazirgh. Siwans, Cabyles, Tuaricks, Guanches.
- Egyptian.
- Semitic.
-
Japetidæ.{
- Occidental.
-
Indo-Germanic.{
-
-
European.{
- Gothic.
- Sarmatian.
- Mediterranean.
- Iranian.
-
-
Our limits will permit us to give a very brief diagnosis only of even the principal of the above divisions, with an indication of their geographical distribution.
1. Mongolidæ. The characteristics of the Mongolian family are to be found in a face broad and flat, from either the development of the zygomata or that of the parietal bones, often from the depression of the nasal bones. The frontal profile is retiring or depressed, rarely approaching the perpendicular. The maxillary profile is moderately projecting, rarely vertical. Eyes often oblique. Skin rarely a true white, and as rarely a true black. The irides are generally dark. The hair is straight, lank, and black, rarely light colored; sometimes curly, rarely woolly. Found in Asia, Polynesia, and America.
According to the above table, the Mongolidae are divided into Altaic, Dioscurian, Oceanic, Hyperborean, Peninsular, American, and Indian.
A. The term Altaic Mongolidæ is derived from the Altai Mountains in Central Asia, as being a convenient geographical point of reference for the nations and tribes comprised in this division. It contains as subdivisions, two principal stocks, the Seriform and Turanian.
The Seriform stock is Mongol in its physical conformation, and is distributed over China, Thibet, the Trans-Gangetic Peninsula as far as Malaya, the Himalayan and parts of the Sub-Himalayan range of mountains.
The principal divisions are: 1. The Chinese, found in China, and having for religion a modified Buddhism, or the religion of Fo. The Chinese, with the yellowish-brown complexion, broad face, scanty beard, lank, black hair, and small stature of the Mongolidae in general, have for their especial characteristic an opening of the eye very narrow, and drawn upwards at its outer angle, so as to render it very oblique. 2. The Thibetans, inhabiting Thibet, Butan, &c. Their religion is chiefly Buddhism, although Brahminism prevails on the frontier of India, and Shia Mahometanism in Little Thibet. 3. The Anamese, in Tonquin and Cochin-China. Their language is allied to the Chinese, although actually different. In physical appearance they resemble the Chinese, although of somewhat less size, and with the eyelids not so oblique. 4. The Siamese, from the Grulf of Siam to the frontiers of China. Their religion is Buddhism. 5. The Kambojians, inhabiting the lower course of the Mekhong Eiver, between the Siamese and Anamese. 6. The Burmese, in the valley of the Irawaddi. 7. The Môn, inhabiting the delta of the Irawaddi, and speaking much the same language as, the Burmese. There are also numerous minor nations which appropriately belong to the Seriform Altaic Mongolidæ.
The Turanian stock inhabits the northern parts of the Chinese Empire, the greater portion of Siberia, Mongolia, Tartary, eastern Turkestan, Asia Minor, Turkey, Hungary, Finland, Esthonia, and Lapland. Four principal divisions may be established, as follows: 1. The Mongolian branch, found from the Altai Mountains to the Wall of China, and from the Tungús boundary to Thibet. Their religion is chiefly Buddhism. It includes the Calmucks, and is characterized by presenting the typical features of the Mongolidæ, and by the pastoral and nomadic habits of its tribes. 2. The Tungus branch. This is found from the Sea of Okhotsk and Kamtschatka to the Yenisei, and from the coast of the ley Sea to the Yellow Sea. Their position is thus more northern than that of the preceding, while their habits are more those of the hunter and lisherman than of the shepherd. 3. The Turk branch, extending from Lake Baikal to the eastern boundary of the Greek and Slavonic countries of Europe, and from the northern frontier of Thibet and Persia to the country north of Tobolsk. They are also found isolated in regions exterior to the preceding limits. Their religion is mostly Sunnite Mahometan. 4. The Ugrian branch. This extends from Norway to the Yenisei, and from the North. Cape to Simbirsk, Saratof, and Astrakhan. It is also found isolated in Hungary. Although essentially Mongolian, there is a frequent occurrence of blue eyes and red hair. Their religion varies in different sections of country, the Lutheran, Roman Catholic, Greek Catholic, and Shaman predominating. The principal nations included in this branch are the Voguls, Ostiaks, Finns, Finlanders, Esthonians, Laplanders, and Magyars or native Hungarians.
B. The Dioscurian Mongolidæ derive their name from the ancient sea-port Dioscurias, where the chief commerce between the Greeks and Romans and the natives of the Caucasian range took place. It includes the nations inhabiting the range of Mount Caucasus, and by authors previous to Latham presented as the type of the Caucasian race, and allied with the inhabitants of civilized Europe. But in the confessed absence of authentic and extended osteological and zoological information, this acute ethnologist, from philological grounds, has felt himself compelled thus to alter the generally received classification. The principal divisions are: — 1. The Georgians; 2. The Lesgians; 3. The Mizjeji; 4. The Irôn; 5. The Circassians.
C. The Oceanic Mongolidæ consist of tribes which, with the exception of those on the Peninsula of Malacca, inhabit islands exclusively. They may be divided into two stocks, Amphinesian and Kelsenonesian.
The Amphinesian stock is sub-Mongolian in physical appearance, with a complexion of various shades of brown or olive, rarely black. The hair is black and straight, rarely woolly; oftener (but not often) wavy and curling. Stature from five feet three to five feet ten. The language contains a certain proportion of Malay words. This stock is distributed over the Malayan Peninsula, the Indian Archipelago, Polynesia, and, perhaps, Madagascar. Its chief subdivisions are: 1. The Protonesians. Here the color is of different shades of brown and yellow. The face is flat; the nose short; eyes and hair black and straight; beard scanty; stature short; frontal profile retiring; jaws projecting; orbits angular. They inhabit the Malayan Peninsula, Sumatra, Borneo, Java, &c. It is here that we find the typical Malays, so well known both for their virtues and their vices. 2. The Pohynesians. This section includes inhabitants of islands from the Pelews to Easter Island, and from the Mariannes and Sandwich Islands to New Zealand. In stature they perhaps exceed the Protonesians, with a more common tendency to corpulence. The color often approaches to that of Europeans; the hair frequently waved or curling; the nose sometimes aquiline. Their diet consists principally of vegetables, the cocoanut, the taro, and the banana; when of animal food, it is chiefly fish, sometimes of pigs and dogs, in the almost entire absence of larger mammals. The bow and arrow are rarely used as weapons, but in their stead the club and spear. Of Polynesians there may be distinguished two branches, those inhabiting the Pelew, Caroline, and Marianne Islands, and those found in the Kavigator, Society, Friendly, and other islands of the Pacific, in the Marquesas, Easter Island, Sandwich Islands, New Zealand, &c.
The Keloenonesian stock has at first sight strong affinities with the black races of mankind, the color of the skin being black, rather than brown or olive. The hair is crisp, curly, frizzly, and sometimes perhaps woolly; scarcely straight; color black. Stature rather small. It inhabits New Gruinea, New Ireland, Solomon’s Isles, the Louisiade, New Hebrides, New Caledonia, Australia, and Tasmania. Here the bow and arrow are the prominent weapons. In this area may be distinguished three principal branches: 1. The Papuan; 2. The Australian; 3. The Tasmanian.
D. The Hyperborean Mongolidæ are found along the coasts of the Arctic Ocean and the courses of the Yenisei and Kolyma, thus occupying the most northern part of the inhabited world. They are constituted by the three divisions of Samoeids, Yeniseians, and Yukahiri.
E. The division of Peninsular Mongolidæ comprises tribes separated by considerable breaks geographically, and to some extent, apparently, ethnologically. Some lie within the Arctic circle, others extend as far south as 26° north latitude, while an equal difference is seen in their social development. They inhabit islands and peninsulas of northeastern Asia. The principal subdivisions are as follows: 1. The Koreans, on the peninsula of Korea; 2. The Japanese; 3. The Lu-Chu Islanders; 4. The Aino; 5. The Koriaks; 6. The Kamtschatkians, in the southern part of the peninsula of Kamtschatka.
F. The American Mongolidæ. These include two principal subdivisions: 1. The Esquimaux, and 2. The Indians of North and South America. The former are not confined to North America, being found in Grreenland and northeastern Asia; the latter constitute exclusively the aboriginal inhabitants of the continent.
G. The Indian Mongolidæ include the inhabitants of Hindostan, Cashmere, Ceylon, the Maldives and Laccadives, and part of Beloochistan.
2. Atlantidæ. In the second great family of mankind we find, as the predominant characters, the maxillary profile projectile, the nose flattened, the forehead retreating, the cranium long, with the parietal diameter generally narrow. The eyes are rarely oblique. The skin is often jet black, very rarely approaching a pure white. The hair is crisp, woolly, rarely straight, still more rarely light-colored. The Atlantidae are almost exclusively inhabitants of Africa, being found in Asia only on the African side. They may be divided into the Negro; the Kaffre; the Hottentot; the Nilotic; the Amazirgh; the Egyptian; and the Semitic Atlantidæ.
A. The Negro Atlantidæ are distinguished by the black, soft, and unctuous skin; the woolly hair; thick lips; projecting jaws; retreating forehead, and flattened nose. They inhabit the low lands and sea portions of Africa, with the delta and courses of the Senegal, Gambia, Niger, Upper Nile, and other rivers of the same continent. Geographically they may be divided into, 1. the Western; 2. the Central; and 8. the Eastern.
B. The Caffre Atlantidæ are subdivided into, 1. The Western; 2. The Southern; and 3. The Eastern, Here the cranium is more vaulted than in the Negro, with the snout less projecting. The hair is tufted, as such approaching the Hottentot; the zygomatic development outwards rather than downwards, so that the cheek bones become projecting, and the forehead and chin tapering. Lips generally thick, and nose less depressed than in the Negro. Color black, dark brown, or clear brown. Stature tall. They occupy western, central, and eastern Africa, from the north of the Equator to the south of the Tropic of Capricorn.
C. The Hottentot Atlantidæ are low of stature and slight of limb. In color they are more brown or yellow than black; cheek bones prominent; nose flattened; hair in tufts rather than equally distributed over the head. Eyes oblique; vision acute. Cranium Mongol-like, with wide orbits; chin long, forward, and thin. There are also striking features in the osteology and general anatomy of the Hottentot, to which we cannot here allude. They inhabit elevated table-lands and terraces, generally sterile and ill adapted to furnish vegetable food. The flesh of the larger mammals, with that of reptiles and insects, is an important article of diet. Their principal divisions are into Hottentots proper and Saabs, the former found on the Great Fish River and Orange River, the latter in the country between the Roggeveld and the middle portion of Orange River.
D. Nilotic Atlantidæ. This division includes the inhabitants of the water system of the Upper and Middle Nile. In external appearance they differ somewhat from the true Negro type, approaching to that of the Arab. They are divided into Gallas, Agows, Nubians, and Bisharis.
E. The Amazirgh Atlantidæ inhabit the north-western portion of Africa, together with a narrow strip along the Mediterranean, from about 15° east longitude to the confines of Egypt. They are interesting as being the descendants of the ancient Gsetulians, Niimidians, Mauritanians, and Cyrenasans. In physical appearance they resemble sometimes the Negro, sometimes the Arab. Their chief divisions are: 1. The Siwans of the oasis of Siwah; 2. The Cabyles of Mount Atlas; 3. The Tuaricks of the Sahara; and 4. The Guanches of the Canary Islands. The latter have now no distinct existence.
F. The Egyptian Atlantidæ. By these are to be understood the old Egyptians, the subjects of the Pharaohs and the Ptolemies, and the modern Copts, as far as they are of unmixed blood. They inhabited and still inhabit the valley and delta of the Nile, from Assouan to the Mediterranean.
G. Semitic Atlantidæ. These are composed of light complexioned tribes, with sub-depressed skulls, straight and prominent noses, and vertical profile. They are referable to three principal types, the Arab, the Jew, and the Kaldani. Their principal divisions are into Syrians, Assyrians, Babylonians, Arabs, Ethiopians, Phoenicians, Jews, &c.
3. The Japetidæ constitute the third and last division of the table prefixed to this article. It is this which includes the majority of the present inhabitants of civilized Europe, and is found in many other portions of the world, originally colonized from Europe. In this family the jaws project but slightly, the nose is mostly prominent, the facial outline sometimes nearly vertical. Face rarely very flat; moderately broad. Eyes rarely oblique. The skin ts white or brunette. Hair never woolly, often light colored. Irides black, blue, or grey. Divided into Occidental and Indo-Germanic.
A. Occidental Japetidæ. The Celts of Brittany, Wales, Highlands of Scotland, the Isle of Man, and Ireland, are the principal representatives of this section. In physical conformation they are presented under two principal types. 1. The Silurian, with eyes and hair black; complexion dark with a ruddy tinge; chiefly found in South Wales. 2. The Hibernian, with grey eyes, yellowish, red, or sandy hair, and light complexion.
B. Indo-Germanic Japetidæ. Of this division we may make two classes, 1. European; 2. Iranian. In the European Indo-Germanic class we find three subdivisions.
1. The Gothic: with blue eyes, flaxen hair, ruddy complexion, smooth skin, and fleshy limbs; or else with grey, dark, or hazel eyes, brown or black hair, and sallow or swarthy complexion. Found at the present time in Germany and Scandinavia, Switzerland, Holland, Belgium, Great Britain, Ireland, United States, Canada, and Australia. Descended from the ancient Germans of the region between the Ehine and the Elbe. It may be divided into the Teutons, having as subdivisions, again, the Moeso-Goths, High Germans, and Low Germans; and into the Scandinavians, including the Icelanders, Faroers, Norwegians, Swedes, and Danes.
2. The Sarmatians, including the Lithuanians (old Prussians, Lithuanians, and Letti), and the Slavonians (Russians, Servians, Illyrians, Tshechs, Poles, Serbs, and Polabi).
3. The Mediterranean, inhabiting Greece and Italy, subdivided into the Hellenic and Italian branches.
The Iranian Indo-Germanic class includes the inhabitants of Kurdistan, Persia, Beloochistan, Affghanistan, and Kafleristan.
The figures on pl. 119 present some of the typical subdivisions to which we have just had reference. Figs. 1 and 2 represent individuals of the German nation; fig. 3, an Arab; fig. 4, a Finn; fig. 5, a Chinese; fig. 6, a true Negro; fig. 7, a North American Indian; fig. 8, a South American Indian; fig. 9, a Malay. Fig. 10, the skull of a Caucasian; fig. 11, that of a Negro; fig. 12, that of an ape. The chart in the centre of the plate is intended to exhibit at a glance the present distribution of the five races of Blumenbach, as explained in the margin. The translation of the German phrases on the plate will be found in the table of contents at the beginning of this volume.
Internal Structure and Vital Phenomena of Man
Investigations in reference to the corporeal nature of man are carried on under two points of view, one having respect to his anatomy, the other to his physiology. By anatomy, is to be understood the structure of the animal machine, with the form and constitution of the individual parts; while physiology, on the other hand, seeks to explain the office or function which each part of the system plays in the animal economy.
Human Anatomy is divisible, in the first place, into General and Special-General Anatomy treats of the minute individual components of the body; their varieties of structure, their peculiarities, and their mode of combination; it stands in very close connexion with the chemistry of the human body Special Anatomy refers to the individual organs, teaching their forms, magnitudes, positions, and connexions with the other parts of the body.
Constituents and Elementary Tissue of the Human Body
The human body consists of solid, liquid, and gaseous substances, so intimately united as to be only separable by artificial means. All solid particles, for instance, are penetrated by liquid, and these contain gaseous in solution. In addition to these, there are cavities in various portions of the body, more or less moistened or filled with collections of liquid matter, not to speak of the gases contained in the lungs, the intestinal canal, &c.
The liquids of the human body constitute its principal mass, amounting to nearly four fifths of the entire weight. They consist in part of a watery matter, generally distributed throughout the body, and containing a little albumen and a few salts in solution; partly of nutritious juices, as the blood, the lymph, and the chyle; and partly of secretions, which are separated from the blood to be entirely thrown off, or else used for some special purpose. Thus we have serous liquids in the cellular tissue, in various closed cavities, in the chambers of the eye, and in the inner ear: albuminous are found in the synovial membranes and the vitreous humor of the eye: fats occur in the cellular tissue and in the marrow of bones: coloring matters in the blood, the muscles, and under the skin of certain races.
All the components of the body may be reduced to fifteen elementary constituents, which, however, are not peculiar to it. These are oxygen, hydrogen, nitrogen, carbon, sulphur, phosphorus, sodium, chlorine, fluorine, potassium, calcium, magnesium, manganese, silicon, and iron.
Some principal organic combinations of these elements in the human body are as follows: tears; saliva; crystalline in the crystalline lens; biliary resin, biliary sugar (bilin), taurine, bilifulvin, cholesterin, dyslysin, &c., in the bile; uric acid and urea in the urine; caseine, whey, butter, sugar of milk, and lactic acid, in milk; mucus; horn, in the epidermis, hair, and nails; fibrine in the blood, lymph, chyle, and muscles; cdbumen in serum, in the substance of the brain and nerves, in the muscles, the synovia, the lymphs, the fluids of the eye, and the ear wax; fatty substances, either separate in the cellular tissue and the cavities of bones, or united with other matters, as in chyle, in the brain, in milk, bile, &c.; osmazome, the substance to which the peculiar smell and taste of roasted meat is due; jelly; hæmatine (coloring matter of the blood); pigmentum nigrum in the eye, the skin of negroes, &c., &c.
The elements of the body, as above enumerated, are combined into various tissues, of which the following are those most generally distinguished: dermoid; cartilaginous; fibro-cartilaginous; fibrous; nervous; osseous; cellular; adipose; vascular; muscular; erectile; mucous; serous; glandular. These various tissues, whose combination constitutes the various organs of the body, will be treated of more fully hereafter. The explanation of the cellular tissue, however, may here find its most appropriate place. This consists of a soft transparent substance, capable of being drawn out into threads, and forming sheets or fascia, in many places rendered opake by a closely compacted web of vascular tissue. It is found beneath the skin; between the different muscles, and even separating their finest fibres; investing, and in part constituting, various organs; in fact there is scarcely any part of the body in which it may not be detected. It is eminently characterized by the presence of cellular cavities, which appear to communicate freely with one another, and thus permit the ready passage of fluids.
Arrarngement of Special Systematic Anatomy
The problem in Systematic Anatomy is to describe the highly various parts of the human body, in such order of succession as shall correspond most nearly to their actual combinations, and most clearly exhibit their various relations and functions. The arrangement which we have fixed on as answering the necessary conditions supposes six general heads, as follows:
- The Bones (Osteology). This has reference to the structure of the central firm basis of the body, the osseous system, a framework inclosed by soft parts, and furnishing cavities which embrace the more delicate organs, as well as constituting a series of levers and fulcra, by means of which the muscles are enabled to bring about extensive and rapid as well as delicate motions.
- The Ligaments (Syndesmology). This includes those parts of the body by means of which the individual bones are so connected together as to permit of relative motions through the agency of the muscles. These two departments are usually treated of under one head.
- The Muscles (Myology). This embraces the muscular system (with its tendons, aponeuroses, and bursæ mucosæ), which operates actively by means of its contractibility, in producing motions in the passive skeleton with its ligaments.
- The Vessels (Angeiology). These consist of the arborescent or reticulated tubes or channels distributed throughout the body, in which the fluids necessary to life, as the blood, the lymph, and the chyle, are kept in constant movement. They include arteries, veins, and lymphatics.
- The Nerves (Neurology). Under this head we treat of the nervous system, a series of tubular sheaths filled with a whitish matter, and united in larger or smaller bundles, which traverse the entire body, proceeding from a central organ of great development, the brain and spinal marrow. Of nerves we distinguish two kinds: the. one conveying impressions from the outer world to the central organs (nerves of sensation); the other serving as the medium for the transmission of volitions (nerves of motion).
- The Viscera (Splanchnology). This subject embraces various complicated organs, adapted to special purposes. Thus, in the head and neck there are the organs of sight, of hearing, of smell, of taste, and of voice; in the thorax, we have the respiratory organs (the lungs) with the thymus and thyroid glands; in the abdominal cavity, the apparatus of digestion (chylopoietic viscera) the urinary apparatus (uropoietic viscera), and the organs of generation.
![]() Anatomy of the Bones and Ligaments (Osteology and Syndesmology)
Anatomy of the Bones and Ligaments (Osteology and Syndesmology)
 Anatomy of the Bones and Ligaments (Osteology and Syndesmology)
Anatomy of the Bones and Ligaments (Osteology and Syndesmology)Articulations of the Human Skeleton
The bones are those hard, compact, and inflexible portions of the body which are inclosed by the muscles, and are united together by ligaments and other modes of attachment into the skeleton. This union may be of such a nature as to permit of little or no relative motion of the two contiguous bones; or, on the other hand, such motion may readily take place by means of synovial joints.
We therefore distinguish two kinds of union among bones, each having various subdivisions, which we shall now proceed briefly to enumerate.
- Synarthrosis. The essential characters of this kind of articulation are: 1. That they are very limited in their motions, so as by some to be considered as immovable; 2. That their surfaces are continuous, or without the intervention of a synovial cavity, but with that of some structure different from bone. The principal varieties are as follows:
- Sutura. This may be either true (vera) as when the margins of two contiguous bones are mutually interlocked in each other, or false (notha), where the bones are in juxtaposition by plane but rough surfaces. Sutura vera may be either dentata, when the processes are long and dentiform, as in the inter-parietal suture of the human cranium; serrata. when the indentations or processes are small and fine like the teeth of a saw, as in the suture between the two portions of the frontal bone; limbosa, when, together with the dentated margins, there is a bevelment, so that one edge rests on the other, as in the occipito-parietal suture. Of sutura notha there are two kinds, squamosa, when the bevelled edge of one overlaps and rests on the other, as in the temporo-parietal suture; and harmonia, where there is simple apposition, as seen in the union of most bones of the face.
- Schindylesis. This second form of synarthrosis is where a thin plate of bone is received into a space or cleft formed by the separation of two laminæ of another bone, as seen in the insertion of the azygos process of the sphenoid bone into the fissure on the superior margin of the vomer.
- Gomphosis. Here one bone is inserted into a cavity in another, just as a nail is driven into a board, or a tree implanted by its roots in the ground. The sole instance in the human subject is seen in the insertion of the teeth in the alveoli or sockets.
- Amphiarthrosis, This is an articulation where two plane or mutually adapted surfaces are held together by a cartilaginous or fibro-cartilaginous lamina of considerable thickness, as well as by external ligaments. By reason of the elasticity of the interposed lamina, the joint possesses a manifest though slight degree of motion. Examples of this form of joint are found in the articulations between the bodies of the vertebae, that between the two bones of the pubes, and that between the ilium and sacrum.
- Diarthrosis. Evident mobility is the distinguishing characteristic of this class of joints; the articular surfaces are contiguous, each covered by a lamina of cartilage (diarthrodal cartilage) having either one or two synovial sacs interposed. The integrity of the articulation is maintained by ligaments which pass from one bone to the other. The varieties are as follows:
- Arthrodia. Here the surfaces are plane, or nearly so: the motion is that of gliding, limited in extent and direction only by the ligament of the joint or by processes of the bones. Examples are seen in the articular processes of the vertebra, in the radial, the carpal, the sterno-clavicular, and other joints.
- Enarthrosis. This, sometimes termed a ball and socket joint, is where the globular head of one bone plays in a cup-like cavity of another, or others. The ball is kept in place by a capsular ligament. Sometimes there passes a straight ligament from the head of the ball to be inserted into the bottom of the socket. An instance of this is seen in the attachment of the thigh bone to the pelvis. The shoulder affords a second instance of the ball and socket joint.
- Ginglymus or hinge joint. Here the articular surfaces are marked with elevations and depressions, which exactly fit into each other, so as to restrict motion in all but one line of direction. They are always provided with strong lateral ligaments, which are the chief bonds of union of the articular surfaces. Perfect examples of this articulation are furnished by the elbow and ankle joints. The knee also, and the phalangeal joints, are true ginglymi.
- Trecharthrosis. A pivot and a ring constitute the mechanism of this form of joint. The ring is generally formed partly of bone and partly of ligament; it sometimes moves on the pivot, and sometimes the pivot moves in it. The motion is confined to rotation, the axis of which is the axis of the pivot. The best illustration of this articulation in the human subject is that between the atlas and odontoid process of the axis or vertebra denlata. Another example is seen in the superior radio-ulnar articulation.
The ligaments which tie the bones together are of two kinds, capsular and funicular. The former resemble a bag open at both ends, in which the extremities of the bone forming the joint are included. The latter are simple cords extending from one bone to another; they may be either cylindrical or flattened. They are variously placed; in some instances they are within the capsular ligament, in others on the outer surface, and sometimes so blended with it as not to be separable without an artificial dissection. The attachment of the head of the thigh bone to its socket in the pelvis illustrates the capsular ligament, while that of the tibia to the thigh furnishes an example of the funicular. Cartilages are also found placed between joints for the purpose of diminishing friction. All the movable articulations also have their surfaces covered with a layer of cartilage of the most exquisite smoothness. In addition to this, there is a closed sac called the synovial membrane, lining the articulation and reflected over the inner faces of the capsular ligament and the articular cartilages. This membrane, unlike the capsular ligament, has no opening whatever. Its whole inner surface appears to secrete the oily fluid called synovia, whose object is to give suppleness and lubricity to the joint.
The human skeleton, considered as a whole, may be conveniently divided into head, trunk, and limbs, all together including from 213 to 217 distinct bones.
Projections on the bones either form articulations with other bones, and are known as head, condyle, &c., or they serve for the attachment of muscles and tendons, in which case they become projections, processes, trochanters, crests, lines, spines, ridges, &c. Depressions, cavities, or fissures are for the attachment of muscles, the formation of articulations, or for the passage of vessels and nerves. They are called furrows, impressions, holes, fissures, canals, grooves, notches, &c.
Bones of the Head
Beginning with the head we find a primary division into the bones of the cranium or skull, and bones of the face.
Bones of the Cranium
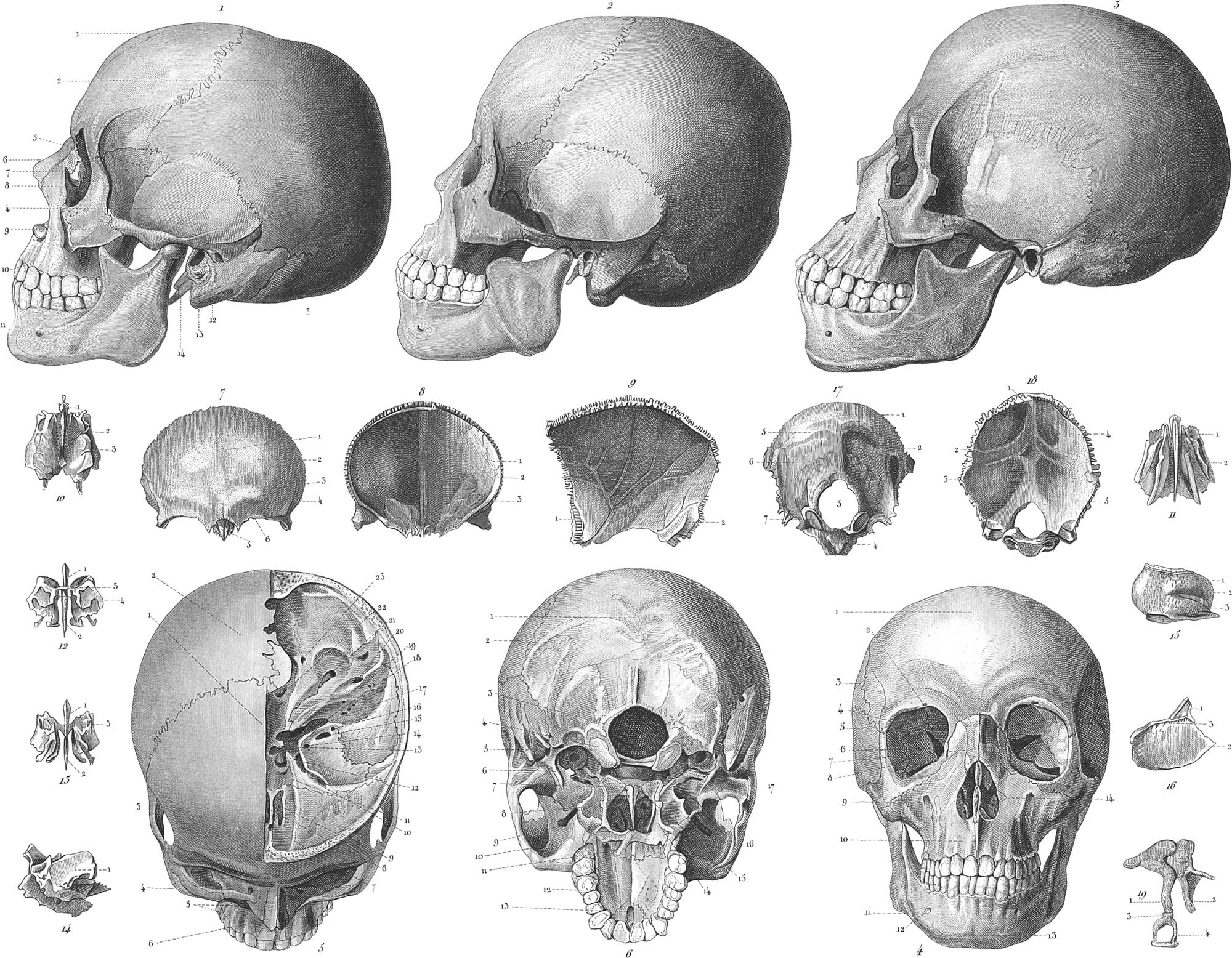
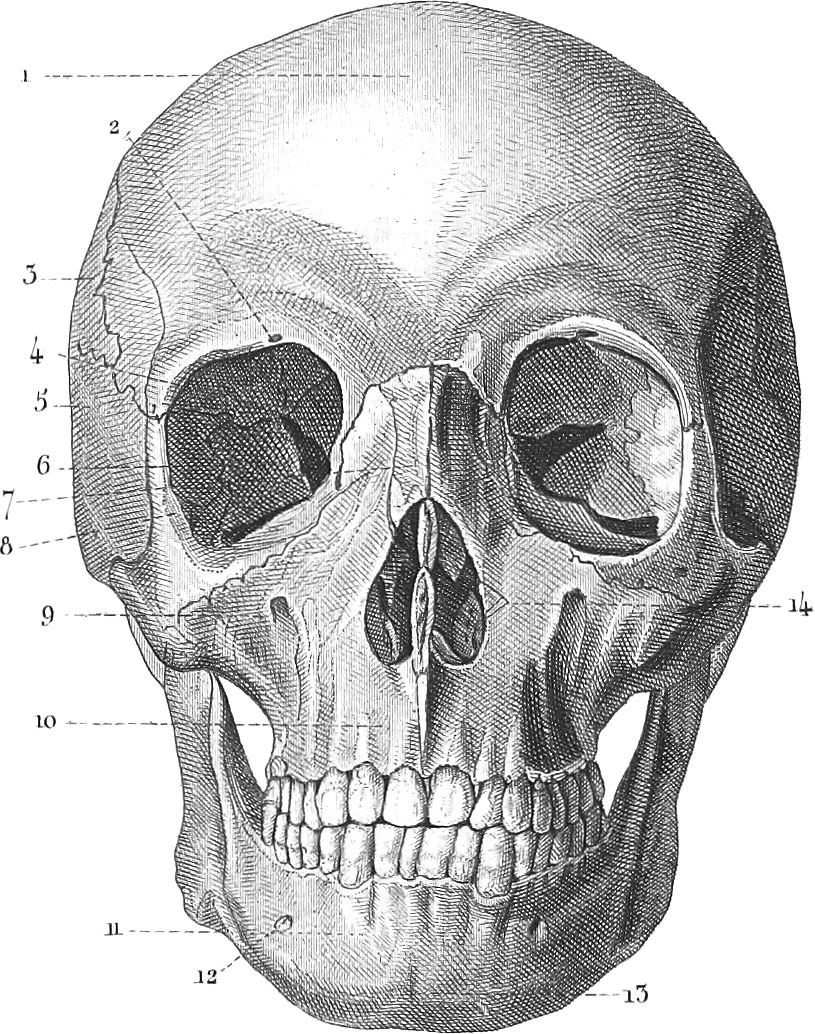
The cranium is composed of eight bones: the os frontis, the os occipitis, the two ossa temporum, two ossa parietalia, the os sphenoides, and the os ethmoides. The first of these, the os frontis or frontal bone, is represented in pl. 121, figs. 11 41, 51 and 7, from the anterior surface, fig. 8 from the interior, and pl. 123, fig. 1, from below. It forms the whole anterior and a portion of the superior lateral and inferior walls of the cranium, and may be divided into the frontal, the two orbitar, and the nasal portions. Between the two tables of the bone are to be found certain cavities or cells called frontal sinuses (pl. 123, fig. 35), lined by a mucous membrane. A median central line on the outer surface shows the line of nnion of the two symmetrical halves into which the bone is divided when young (pl. 121, fig. 71); this line is often replaced, especially in the young, by a suture called the frontal suture. The frontal protuberances (fig. 72) over the eyes mark the centres of ossification in the fœtus: the superciliary ridges (fig. 73) below these serve for the attachment of the muscle for wrinkling the eyebrows. Nearly in the middle of the upper-orbitar border is a foramen or notch (fig. 42, 76), the supra-orbitary foramen for the passage of the supra-orbital artery, veins, and nerve. The inner face of the bone is strongly marked by depressions corresponding with the convolutions of the brain, and also caused by impressions of bloodvessels (fig. 81,2,3). On its middle exists a vertical ridge becoming more elevated as it approaches the ethmoid bone, and terminating below in the foramen cœcum (fig. 57), occupied by a process from the great falx of the dura mater as well as by some very small veins. At the exterior angular part of the orbitar process of the frontal bone is a depression for receiving the lachrymal gland and called the lachrymal fossa (pl. 123, fig. 13); on the nasal side there is a smaller depression or a small spine, fossa or spina trochlearis (fig. 14), serving as a pulley for the superior oblique muscle of the eye. Separating the two orbitar processes, is a large notch for receiving the cribriform plate of the ethmoid bone (fig. 11), and on each side of this are cells (fig. 15), which are continuous with those of the ethmoid.
The parietal bones, ossa parietalia (pl. 121, fig. 12, fig. 43, fig. 52, fig. 9, interior surface). These bones are quadrilateral, convex externally, concave internally. They constitute the superior and lateral portions of the middle of the cranium, abutting against each other along its median line. Externally they are smooth, but raised about their middle into the parietal protuberances, the centres of ossification; below these protuberances there is an arched, broad, but slightly elevated ridge for the attachment of the temporal fascia and muscle, and continuous with the ridge on the side of the frontal bone. The internal surface is marked by the convolutions of the brain, and also exhibits a number of arborescent furrows produced by the ramifications of the middle artery of the dura mater (pl. 121, fig. 91). At the inferior posterior corner of the bone there is also a fossa, which is made by the lateral sinus of the dura mater (fig. 92).
The occipital bone, os occipitis (pl. 121, fig. 13, fig. 61, fig. 17, external surface; fig. 18, internal). It forms part of the posterior and inferior walls of the cranium, and when anchylosed with the sphenoid, as is usually the case in advanced age, constitutes the basilar bone, os basilare. On the posterior external surface, and half-way between the foramen magnum and the upper angle of the bone, is seen the occipital protuberance, from the lower part of which a small vertical ridge is extended towards that foramen. Into this ridge is inserted the ligamentum nuchæ. From either side of the protuberance an arched ridge extends to the lateral angle of the bone, known as the superior semi-circular ridge or line; in addition to these we see another ridge and various cavities (fig. 171,2,5,6) for the attachment of muscles. In the lower section of the bone is the foramen magnum (pl. 121, fig. 173), through which pass the medulhi oblongata, the vertebral arteries and veins, and the spinal accessory nerves; on each side are seen the condyles (fig. 64, 177) or surfaces of articulation between the head and the vertebral column, constituting a hinge-joint by which the former may be moved backwards and forwards. In a depression behind each condyle is the posterior condyloid foramen, which conducts a cervical vein to the lateral sinus. There is likewise the anterior condyloid foramen for conducting the hypoglossal nerve to the tongue. On the interior surface, behind the foramen magnum, is seen a rectangular cross (fig. 181,2), forming at the centre the internal occipital protuberance. To this cross the dura mater is attached, and it also exhibits the impressions of cerebral bloodvessels. In the angles of the cross are seen broad concavities, the two superior of which receive the posterior lobes of the cerebrum, and the two inferior those of the cerebellum (fig. 184,5).
Anterior to the lower part of the occipital bone, and placed transversely in the-middle of the base of the cranium, is the sphenoid bone, os sphenoideum (pl. 122, fig. 6 above, fig. 7 below). In the middle of this highly complicated bone is seen the body or centrum, which is hollow and contains the sphenoidal sinuses (pl. 123, fig. 23, fig. 32), communicating with the nose. A deep depression on the upper surface, bounded anteriorly and posteriorly by projecting spines and ridges, is the sella turcica for the reception of the pituitary gland (pl. 122, fig. 61). The inferior surface presents a longitudinal rising in the middle called the sphenoidal or azygos process (fig. 71), for articulation with the vomer. From the upper anterior part of the body arise, one on each side, the apophyses of Ingrassias, the ensiform processes or the little wings (fig. 64), with the bases perforated by the foramen opticum for transmitting the optic nerve with the ophthalmic artery. The two great wings, alæ magnæ (fig. 73,4), arise from the sides of the body by a small irregular base. They present three faces: one anterior, called orbital from its forming part of the orbit; one external, called temporal; and a third turned towards the brain, forming part of the fossa, for containing its middle lobe. Between the great and the small wings is a considerable fissure called foramen sphenoidale, or foramen lacerum superius (fig. 66), for transmitting the third, fourth, sixth, and first branch of the fifth pairs of nerves and the ophthalmic vein. Below the base of this hole is the foramen rotundum (fig. 67) for the passage of the second branch of the fifth pair, and behind the foramen rotundum again, is the foramen ovale (fig. 68) for the exit of the third branch of the fifth pair. About two lines behind the foramen ovale is the foramen spinale (fig. 69) for transmitting the middle artery of the dura mater.
From the lower part of the two great wings project downwards on each side the two pterygoid processes constituting the posterior portion of the mouth (fig. 67). They serve for the attachment of certain muscles, and are pierced at their base by the pterygoid foramen for transmitting the nerve of the same name.
The sphenoid bone articulates above and in front with the vomer, the frontal, ethmoidal, malar, and parietal bones, laterally with the temporal, behind with the occipital, and by the pterygoid processes with the palatine bones.
Temporal bones, ossa temporum (pl. 121, fig. 14, 12, 13, 14; pl. 122, figs. 8, 9). These bones form portions of the inferior lateral walls and of the base of the cranium. They articulate with the occipital, the parietal, the sphenoid, inferior maxillary, and the malar. Their figure is very irregular, consisting of three portions, the squamous, the petrous, and the mastoid.
The squamous portion (pl. 121, fig. 14) is the thin circular and anterior part which forms the inferior portion of the temples. The exterior surface is smooth and slightly convex, the interior is formed into fossæ by the convolutions of the brain. The greater portion of the circumference of the squamous portion is bevelled for articulation with the parietal and sphenoid bones; at the anterior inferior part, however, it is serrated and thicker. On the exterior of this portion is the glenoid cavity (pl. 122, fig. 84) for articulating with the lower jaw. The outer margin of this cavity is constituted by the base of the zygomatic process (fig. 82), which extends forwards to join the malar bone.
The mastoid portion (pl. 121, fig. 112, fig. 87) is thick and cellular, the upper portion being received between the parietal and occipital bones. The cells known as the mastoid sinuses communicate with the tympanic cavity. We also distinguish a mastoid process for the attachment of the sterno-mastoid and trachelo-mastoid muscles; together with a mastoid foramen, for the passage of a vein into the lateral sinus.
The petrous portion of the temporal bone (pl. 121, fig. 113, 14; pl. 123, fig. 91, 2) is a triangular pyramid, arising from the inner side of the mastoid and squamous portions. In the posterior surface of the petrous bone is the meatus auditoriws internus (fig. 32), for the transmission of the seventh or auditory and the facial nerve. Between the mastoid and zygomatic processes is the meatus auditorius externus (fig. 85), which leads to the tympanum. Its rough lower margin is called the auditory process, and to it is attached the cartilage of the external ear. The styloid process for the attachment of the styloid muscles is seen in fig. 93. Behind the root of this process is the stylo-mastoid foramen, which transmits the facial nerve to the face. The jugular fossa, which is situated within the styloid process and the foramen, is occupied, in conjunction with a similar one in the occipital bone, by the internal jugular vein, and the eighth pair of nerves. Anterior to the lower end of this fossa is the foramen caroticum, through which passes the carotid artery and the upper extremity of the sympathetic nerve. The orifice of the eustachian tube is to be found in the angle between the squamous and petrous parts, mthin the glenoid foramen.
The ethmoid bone, os ethmoides (pl. 121, fig. 10, from above; fig. 11, from below; fig. 12, from behind; fig. 13, from before; fig. 14, from the orbitar side; 15, from the nasal or inner side; fig. 16, the septum). This bone is so placed as to fill the vacancy between the orbitar processes of the frontal bone. It is cuboidal, and highly cellular. The only part which looks towards the brain is the cribriform plate, lamina cribrosa (fig. 102), with a vertical median ridge or process called the crista galli (figs. 10, 12, 13, 161). This plate is perforated by numerous lioles, through which pass the ramifications of the olfactory nerve. The lateral portions of the ethmoid (pl. 121, fig. 103) are covered by the frontal bone. That portion of the ethmoid which enters into the orbitar cavity (fig. 141) is called the os planum, or lamina papyracea. The internal or nasal face forms part of the nostril. Between the two halves of the bone, and beneath the cribriform plate, is the nasal lamella, or lamina perpendicularis (fig. 111, 123, 132), which, in conjunction with the vomer, divides the nasal cavity into halves. In the posterior middle portion of the nasal face is a deep furrow, called the superior nasal meatus (fig. 152). The upper margin of this meatus is constituted by the upper turbinated bone, the middle turbinated bone being below.
Bones of the Face
The face is composed of fourteen bones, of which thirteen enter into the composition of the upper jaw. Of these, twelve are in pairs: the ossa maxillaria superiora, ossa malarum, ossa nasi, ossa ungues, ossa turbinata inferiora, ossa palati. The single vomer constitutes the thirteenth, and the os maxillare inferius, or lower jaw, the fourteenth.
Superior maxillary bones, ossa maxillaria superiora (pl. 121, figs. 110, 410; pl. 123, fig. 6). These are the largest of the bones of the face, and occupy the anterior part of the upper jaw. Each consists of a central portion, with various processes for articulation with the contiguous bones. This central portion is hollowed out into a large cavity, called the antrum highmorianwn, or maxillary sinus, communicating with the cavity of the nose. The superior face is formed by a thin plate, the orbitar process, constituting the floor of the orbit (pl. 123, fig. 63). In the posterior part of this plate is a groove, which leads to a canal terminating at the front of the bone in the infra-orbital foramen (fig. 64; pl. 121, fig. 49), through which pass the infra-orbital nerve and an artery; below this, again, is a depression in the front of the bone (pl. 123, fig. 63), known as the fossa maxillaris, filled up during life by muscle and fat. The nasal process (fig. 61,2) connects the bone with the frontal and nasal bones, and exhibits an emargination inferiorly and anteriorly (fig. 62), to which is attached the cartilage of the nose. The malar or zygomatic process (fig. 67) connects it with the malar bone. The alveolar processes, for lodging the eight teeth of the adult, are situated in the external inferior portion, and the palatine process (pl. 121, fig. 612) constitutes the greater portion of the bony palate. In the suture of the two maxillary bones, and immediately behind the front alveolar processes, we find the foramen incisivum (fig. 613), which bifurcates above, sending a branch into each nostril. Through this passes a branch of the spheno-palatine nerve. The intermaxillary bone, so universal in the lower Mammalia, is wanting as a distinct element in the adult man (it being fused with the true maxillary), but in the young fœtus may be distinctly recognised; it rarely exists after birth. The articulations of the maxillary bones are with the frontal, nasal, unguiform, malar, and ethmoid, above; with the palatine, behind; with the vomer, in the middle; and with the inferior spongy bone, by the nasal surface.
Palate bones, ossa palati (pl. 123, fig. 7, from without; fig. 8, from within; and fig. 9, from behind). These bones, two in number, are placed posterior to the maxillary, between them and the pterygoid processes of the Sphenoid. For this reason, they are but slightly conspicuous in the entire skull. The palate plate of these bones forms the posterior continuation of the palate process of the superior maxillary in the bony palate (pl. 121, fig. 611).
The nasal plate, or ascending portion, constitutes the posterior external part of the nostril. The upper extremity is formed by two processes, one anterior, the other posterior; and separated by either a round notch or by a foramen. The posterior of the two is known as the pterygoid apophysis.
The orbitar portion is irregular in shape, and may be seen between the ethmoid and maxillary bones, in the back part of the orbit. The sphenopalatine foramen is the notch between the orbitar portion and the pterygoid apophysis, completed into a foramen by the application of the sphenoid bone. Through this passes the lateral nasal nerve, with the spheno-palatine artery and vein. There are various grooves and canals in the palate bones, which, continuously with corresponding grooves in other bones, transmit vessels and nerves to the soft palate (pl. 123, fig. 71, 93).
The palate bones articulate each with its fellow, on the opposite side of the median plane of the face; also with the upper maxillary, the. sphenoid, the ethmoid, the inferior spongy, and the vomer.
The nasal bones, ossa nasi (pl. 121, fig. 16; fig. 47; fig. 56; pl. 123, fig. 10, a). These bones, two in number, are situated between the nasal processes of the superior maxillaries. They are oblong in shape, and are applied to each other so as to constitute a strong arch, called the bridge of the nose. They also articulate with the frontal bone above.
The unguiform or lachrymal bones, ossa lachrymalia, ungues (pl. 121, fig. 17; pl. 123, fig. 11). This bone is placed at the internal side of the orbit, and constitutes the nasal duct for the tears, by its application to a process of the inferior turbinated bone.
The inferior spongy bones, ossa conchæ inferiora (pl. 123, fig. 14). This bone is situated at the inferior lateral part of the nose, just below the opening into the maxillary sinus. The anterior extremity rests upon the ridge across the root of the nasal process of the upper maxillary. The posterior extremity rests similarly upon the ridge across the nasal plate of the palate bone.
The vomer or ploughshare, vomer (pl. 121, fig. 615; pl. 123, fig. 13). This single bone constitutes the lower portion of the bony septum of the nostrils. The superior broader margin has a furrow for receiving the azygos process of the sphenoid bone. The posterior margin is rounded and smooth. The inferior margin articulates with the spine or ridge of the superior maxillary and palate bones.
The cheek or zygomatic bones, ossa malarum (pl. 121, fig. 19; pl. 123, fig. 12). These bones are situated at the external part of the orbit, and constitute the middle external part of the face. Of the three surfaces, the one which enters into the orbit is known as the internal orbitar process. The front surface is convex and belongs to the bones of the face; the third surface is concave and forms part of the zygomatic fossa. Of the processes of this bone, the upper one is the superior orbitar. The orbitar margin terminates inferiorly in the inferior orbitar or angular process. The zygomatic process joins the bone with the zygoma of the temporal bone; the maxillary bone forms a fourth angle.
This bone articulates with the maxillary, the frontal, the sphenoidal, and the temporal.
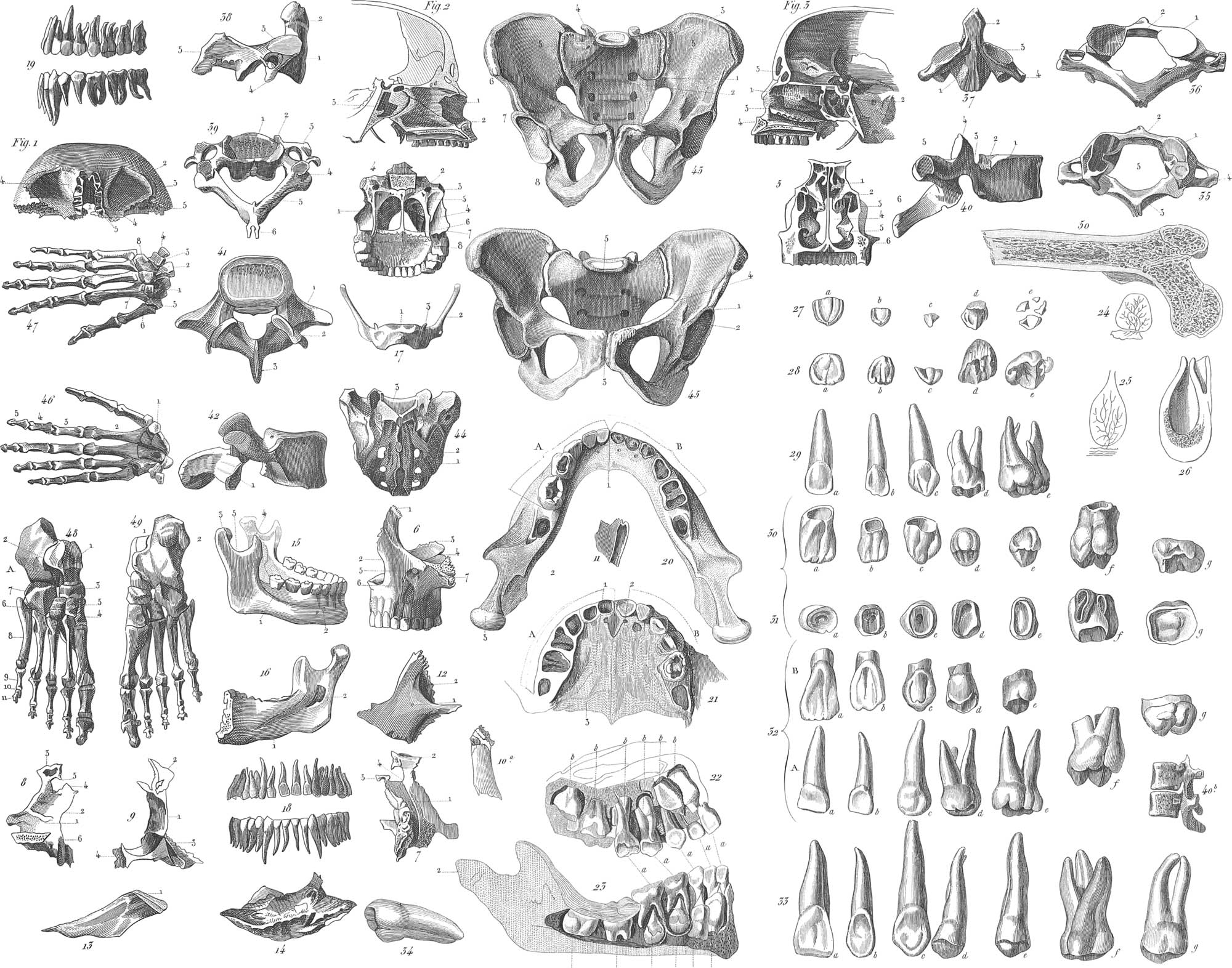
Lower jaw, maxilla inferior (pl. 123, figs. 15, 16). This bone articulates freely with the skull by means of the condyloid processes which play in the glenoid cavity of the temporal bone. It is distinguished into the body and the branches. The body consists usually of two halves, which are separate in the very young individual, and unite at the anterior symphysis. In the adult there are sixteen alveoli or sockets for teeth in the superior margin, and the portion thus occupied possesses somewhat the form of a horse shoe. The symphysis corresponds to the chin, mentum (pl. 121, fig. 111, fig. 413), on each side of which is the foramen mentale (pl. 123, fig. 152, pl. 121, fig. 412); through this pass blood-vessels and a nerve to the face. On the inner surface, about the middle, is a small spine, spina mentalis interna, for the attachment of muscles of the tongue and larynx. The extremities of the lower jaw, rami, are quadrilateral, and rise up much above the level of the body. The superior margin of each ramus exhibits a crescentic notch dividing it into two portions. The anterior portion is triangular and slightly curved backwards; to it is attached the temporal muscle, and it is known as the coronoid process (pl. 123, fig. 154). The posterior border of the notch or concavity is constituted by the condyloid process (fig. 153), the application of which has already been mentioned. On the inside of each ramus is seen the posterior mental foramen (fig. 162), through which pass the inferior maxillary vessels and nerve.
The lower jaw is articulated with the temporal bone in such a manner as to admit of considerable freedom of motion in an antero-posterior and lateral, and still more in a vertical direction (pl. 124, figs. 1, 2, 3). An interarticular cartilage is placed in the joint for greater freedom of movement (fig. 31). On each side of this cartilage is a synovial membrane separating it from the two faces of the joint. The external lateral ligament (fig. 11) arises from the inferior margin of the root of the zygomatic process of the temporal bone, and is inserted into the neck of the condyloid process. The internal lateral ligament (fig. 21) arises from the spinous process of the sphenoid bone, and is inserted into the spine bordering the posterior mental foramen. The stylo-maxillary ligament (figs. 1, 2, 32) passes from the external side of the styloid process, and is inserted into the posterior margia of the jaw, near its angle.
General Considerations respecting the Head
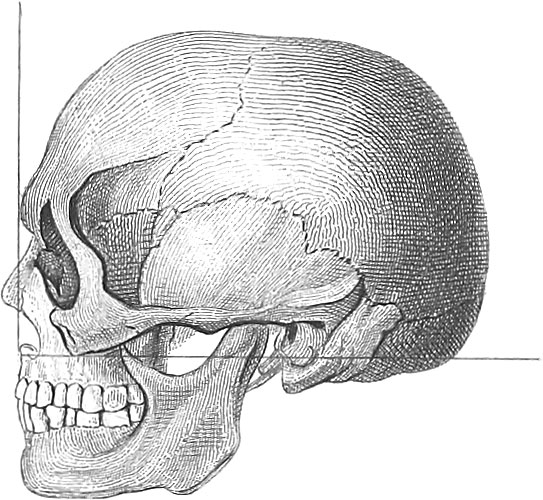
The individual bones hitherto considered constitute the head by their apposition, and, as already remarked, are grouped into bones of the cranium, or brain case proper, and bones of the face. The cranium is an ovoidal case with a flattened base, inclosing a cavity of similar shape, cavum cranii (pl. 121, fig. 5), narrowest anteriorly, but wider in the middle than behind. The precise shape of the cranium, however, depends upon that of the brain, and consequently varies with the individual. In the face are found the orbits or cavities for the eyes, those for the nasal apparatus, and the mouth.
The bones of the skull are mostly united by the articulation known as the sutura. The coronal suture joins the frontal bone with the two parietal, and extends from one temple to the other across the skull. The frontal suture is not always seen, as it usually becomes obliterated with age. When present, however, it extends along the upper median line of the cranium, from the base of the nose to the coronal suture, and divides the two frontal bones. The sagittal suture unites the two parietal bones along the median line in the continuation of the frontal suture, and extends from the coronal to the lambdoidal suture. This lambdoidal suture unites the occipital to the parietal bones by its upper half, and the occipital to the temporal by the lower. The squamous suture unites the temporal to the parietal bones, and occupies the side of the head.
The outer surface of the head may be conveniently divided into four regions. The superior, or the vertex, is smooth and even, without any remarkable features attending it. The lateral regions are each divided into two, the anterior or temporal, and the posterior or mastoid; the meatus auditorius externus is between the two. The inferior region extends from the nasal notch in the frontal bone to the occipital protuberance, and is bounded laterally by the zygomatic arches and by a ridge which is continued from these processes around the skull with but little interruption. This region may be divided into three portions, anterior, middle, and posterior. The anterior basilar region extends from the superciliary ridges of the frontal bone to the roots of the pterygoid processes of the sphenoid; it presents the nasal spine and process of the os frontis, bounded by their angular processes before and by the orbital plates of the sphenoid behind. In this division are the supra-orbital, the anterior and posterior orbital holes, the openings of the frontal and ethmoidal cells, the optic and lacerated foramina of the orbits, the vidian canals, and the foramina rotunda. The middle division extends from the roots of the pterygoid to the styloid processes of the temporal bones; it presents the; azygos process of the sphenoid, the basilar process of the occipital, the anterior points of the petrous portion of the temporal bones, the spinous processes of the sphenoid, and the glenoid cavities of the temporal bones. The foramina, or holes in this division, are the ovale, spinale, carotidum, auditorus externus, and the glenoid; the eustachian canals are external to it. The posterior division extends from the styloid processes of the temporal to the tuberosity of the occipital bone; it presents the foramen magnum, the two condyles, the jugular ridges, the styloid processes of the temporal bones, surrounded by the vaginal processes, the mastoid processes, the digastric grooves, the inferior and superior transverse arches, the spines, protuberance, and depressions of the occipital bone. The foramina in this division are the stylo-mastoid, mastoid, magnum, lacera postica, anterior and posterior condyloid, aqueduotus cochleæ, and the tympanic foramina in the petrous bone.
The inside of the skull (pl. 121, fig. 5) is divided into the arch or vault, and the base. On the vault is seen the sulcus for the longitudinal sinus, the frontal crest, the grooves for the middle arteries of the dura mater, the depressions for the convolutions of the brain and for the granulations or glands of Pacchioni. The base of the skull is very uneven, and presents on each side of the median line three regions or fossæ, on different planes, viz. the anterior or frontal, the middle or spheno-temporal, and the posterior or occipital.
The anterior or frontal division is formed of the orbital plates of the frontal bone, the cribriform plate of the ethmoid, and the lesser wings of the sphenoid. The foramina are the cœcum (fig. 57), the olfactory (fig. 59), the internal orbital, and the optic (fig. 511).
The middle or spheno-temporal division is bounded before by the lesser wings of the sphenoid bone; on the sides by the squamous portions of the temporal, and behind by the superior angles of the petrous portions of the same bone, and by the posterior clinoid processes of the sphenoid. In the middle is the sella turcica; on each side of, but below this, is a groove for the carotid artery (fig. 518), and below this is a shallow groove for the superior maxillary nerve. Further out on each side are the cavities to lodge the middle lobes of the brain, and on the superior surface of the petrous bones are seen the juttings of the vertical semicircular canals. The foramina in this division are, the foramina lacera orbitalia superiora, rotunda (fig. 514), ovalia (fig. 515), carotica (fig. 517), spinalia (fig. 516), lacera basis cranii anteriora, and innominata or hiatus Fallopii.
The posterior or occipital region is bounded before by the basilar process and by the posterior surface of the petrous bones, and behind by the occipital; it presents the basilar process, the foramen magnum, and the perpendicular ridge of the occipital crossed by the transverse, by which this bone is divided into four fossæ. On the superior angle of each petrous bone is a shallow groove for the superior petrosal sinuses; the transverse occipital ridge presents a deep groove for the lateral sinuses, which last are continued over the inferior angles of the parietal bones, and thence descend inwards along the mastoid jDortions of the temporal bones, and then again groove the occipital, passing forwards on it to the posterior foramina lacera. The perpendicular ridge is grooved above for the longitudinal sinus, which terminates sometimes in the left, but more frequently in the right lateral sinus. The vertical ridge below the tentorium gives attachment to the falx minor, and is slightly grooved for the occipital sinuses. The foramina in this division are, the foramina auditoria interiora (fig. 520), the aqueductus vestibulorum, foramina lacera postica, foramen magnum, foramina condyloidæ antica (fig. 522), and postica (fig. 523).
Special Anatomy of the Spine
Bones of the Trunk
The trunk is constituted by the vertebral column or spine, the thorax, and the pelvis.
The spine, columna vertebralis, rachis (pl. 122, fig. 31, 41,3,5, fig. 5, a, b, c), is placed at the posterior part of the trunk, and consists of twenty-eight or twenty-nine pieces. Of these, twenty-four are called true vertebræ, and connected by ligaments so as to form one strong but flexible column. The twenty-fifth piece, reckoning from the head, is the sacrum, and is inserted between the ossa innominata; the remaining three or four constitute the os coccyx, and in their imperfect form represent the caudal vertebræ or tail of other vertebrate animals.
Each vertebra consists of a body, and of several projections or processes. The body occupies the anterior central part; it is thick and spongy, and rather circular or oval; its upper and lower surfaces are flat or slightly concave, and give attachment to the inter-vertebral ligaments. The margin of each is tipped with a compact white substance, and the lower surface is rather larger than the upper. Anteriorly it is transversely convex and grooved horizontally, particularly on either side, and is likewise very porous. Posteriorly it is concave, so as to form part of the spinal canal or foramen. This surface is perforated by large foramina for the escape of the venous canals which ramify through the bone. The processes of each vertebra are nine, two lateral or the laminæ, two transverse, four oblique or articulating, and one spinous.
The lateral processes, or laminæ, arise one on each side, by a sort of pedicle, from the posterior part of the body; they pass backwards, bounding the sides of the spinal hole, and unite posteriorly in the spinous process; they are broad behind, but narrow where they join the body, being grooved out above and below into a notch. The inferior of these is the larger. The laminæ form the lateral and posterior portions of the spinal arch or forameft for the spinal cord. The roots of these laminæ, or the pedicles, are considered by some as separate portions; they form the common point of support for the other processes, and separate the superior from the inferior notch. These notches, where the vertebræ are joined, form the inter-vertebral holes for the passage of the spinal nerves.
The spinous process is the most projecting part of the vertebra in the posterior median line; its base is bifurcated, and passes into the two laminæ; its apex generally ends in a point or tubercle. The whole series of these processes presents the longitudinal prominent crest posteriorly, named spine. Each process receives the insertion of tendons, and serves as a lever for the extensor muscles of the column.
The transverse processes arise from the roots of the laminæ, or rather from the pedicles, and are directed outwards on each side; they serve for the attachment of tendons, and in the dorsal region they also support the ribs.
The articular or oblique processes are four in number; they arise from the roots of the transverse processes or from the pedicles; two ascend, two descend. They are covered with cartilage, and articulate with the corresponding processes of the adjacent vertebræ. The two superior are directed more or less backward, and the two inferior more or less forward; their direction is rather vertical or contrary to that of the surface of the bodies, beyond the level of which they extend, so that their articulations correspond to the inter-vertebral ligaments.
The spinal hole or canal is bounded by the body and processes; it is more or less triangular.
The vertebræ are divided into three sets, all differing in size and shape. The first set reckoned from below is the lumbar (pl. 122, fig. 5 c), consisting of the five bones immediately above the sacrum and at the lower extremity of the column. They are the largest of all. The dorsal (fig. 5 b) are twelve in number, and are situated above the lumbar. They are intermediate in size between the lumbar and the cervical. On each side of the body of a dorsal vertebra there is a notch in the upper and lower margin. When two vertebræ are conjoined, the inferior notch of one is in apposition with the superior notch of the vertebra beneath, and the two notches together constitute an oval depression for the head of a rib.
The cervical vertebræ (fig. 5 a), seven in number, are the smallest of all, and occupy the top of the column. The first or uppermost of all is called the atlas (pl. 123, figs. 35, 36); it consists merely of a bony ring, without a distinct body or spinous process. The laminæ are thick and round behind, but near the articulating processes they are flattened and grooved above for the vertebral artery and first cervical nerve, and below for the second cervical nerve. Before these notches are the articular processes, which receive the occipital condyles. The second vertebra of the neck is known as epistropheus (fig. 37). It is remarkable for the depth of its body, from the upper part of which rises a large round dentiform (odontoid) process (fig. 372), the fore part of which is received into the small articulating cavity on the anterior arch of the atlas, while posteriorly it presents a small, smooth convexity, which moves against the smooth surface of the transverse ligament of the atlas.
Pl. 123, fig. 35, the atlas from above: 1. Superior articular surface for the occipital condyles; 2. Posterior, and 3, anterior arch, with their respective tubercles; 4. Transverse process; 5. Spinal hole.
Fig. 36, the atlas from below: 1. Inferior surfaces for articulating with second cervical vertebra; 2. Articulating surface for the odontoid process of the epistropheus.
Fig. 37, the second cervical vertebra (epistropheus) from behind: 1,the body; 2, odontoid process; 3, superior oblique process; 4, transverse process. Fig. 38, the same from the side: 1, body; 2, odontoid process; 3, superior oblique process or articulating surface; 4, transverse process; 5, spinous process.
Fig. 39. A cervical vertebra from above: 1,2, body; 3, transverse process; 4, oblique process; 5, arch; 6, spinous process.
Pl. 123, fig. 40. A dorsal vertebra from the side: 1, body; 2, articulating face for the head of a rib; 3, intervertebral notch; 4, oblique process; 5, transverse process; 6, spinous process.
Fig. 41. A lumbar vertebra from above: 1, transverse process; 2, oblique process; 3, spinous process. Fig. 42. The same from the side: 1, inferior oblique process.
The sacrum (figs. 43, 44) is a broad flattened triangular bone, concave anteriorly, convex posteriorly, inserted like a wedge between the two ossa innominata, and articulating with the lumbar vertebra above, with the coccyx below. In the young skeleton it is clearly seen to consist of five distinct vertebræ, which become fused together or anchylosed with age, always, however, leaving traces of the original separation, especially on the anterior face. In fact, all the elements of true vertebræ are here present, although in no high condition of development. The upper anterior projecting edge of the sacrum is termed the promontory, behind which is the triangular aperture of the sacral or spinal canal. On either side of this canal is the oblique or articular process. The inferior extremity of the sacrum, or the apex, is directed downwards, sometimes a little forwards; it presents a small transverse, oval, convex surface, for articulation with the coccyx. The anterior concave surface is marked by four transverse lines (fig. 432), at the extremities of which on each side are four large holes (the anterior sacral). These transmit the anterior sacral nerves, veins, and arteries. The posterior surface is roughened by four horizontal eminences in the median line, corresponding with the spinous processes. On each side of this median ridge is a rough groove, in which are four posterior sacral foramina (fig. 442), which transmit the" posterior sacral nerves and some bloodvessels. The inferior extremity of the sacral canal is bounded posteriorly by a ligament, and laterally by two tubercles, cornua sacralia, which descend to meet similar processes from the coccyx.
The ossa coccygis or coccyx (pl. 122, fig. 31) correspond to the caudal vertebræ of animals. They consist of three or four, rarely of five pieces, which in the young are divisible iuto three parts, while in the adult they are united into one or two. Considering the combination into one piece, this in the adult is of triangular shape, serving to prolong anteriorly the curve of the sacrum (fig. 51). The base above is broad, and bounded by two cornua (fig. 311), which interlock with those of the sacrum.
Articulations and Ligaments of the Spine
Articulation of the head with the spine (articulus capitis). This is a double arthrodia, the condyles of the occipital bone being received into the superior oblique processes of the atlas. The motion is quite limited, and restricted almost entirely to a forward and backward movement of the head. The capsular ligament on each side arises from the circumference of the condyle, and is inserted into the circumference of the glenoid cavity of the atlas. The interior of each capsule is lined by a synovial membrane. Anterior and posterior occipito-atlantal ligaments (pl. 124, fig. 41, fig. 51,2) arise from the edges of the foramen magnum, and are inserted into the upper border of the atlas before and behind its oblique processes. The lateral ligaments extend as strong cords from the transverse processes of the occipital bone to those of the atlas.
Between the atlas and occiput, as already remarked, scarcely any motion but that of flexion and extension can occur. The turning of the head, or the horizontal motion, takes place between the first and second vertebræ (the atlas and epistropheus). To this end, the articular extremity of the odontoid process rests on a depression on the posterior border of the anterior arch of the atlas. It is held in this position by a capsular ligament, but for the sake of greater security a strong, straight ligament (the transversal) extends behind it from one side of the atlas to the other. The neck of the odontoid process is thus inclosed in a circular collar, formed by the arch of the atlas in front and the transverse ligament behind, in which it can rotate like a pivot, being held most securely in its place (pl. 124, fig. 73). The importance of this ligament is very great; in cases where it has become softened by disease, and ruptured, death has been instantaneous; the head falling forward and the odontoid process projecting backward, has either compressed or pierced the medulla oblongata. An additional security against dislocation is furnished by the moderator or check ligaments, lig. suspensorium dentis epistrophei (fig. 71,2), which arise one from each side of the odontoid process, and are inserted into a depression on the inner side of each occipital condyle. The two ligaments are usually united by a fasciculus which passes above the summit of the odontoid process. In addition we find a ligament, the middle occipito-axoid or apparatus ligamentosus (fig. 51), extending from the inner surface of the basilar process of the occipital bone beneath the dura mater, and passing through the foramen occipitale, to be inserted into the superior part of the transverse ligament of the atlas, and below this into the bodies of the second, third, and fourth vertebræ.
In addition to the ligament extending between the head and first and second cervical vertebræ, there are others which either extend continuously along the entire spine, or are repeated between each contiguous pair of vertebræ. These may be distinguished into two sets: those which unite the bodies, and those uniting the processes. The first comprise the anterior and posterior common vertebral ligaments and the intervertebral fibro-cartilages or ligaments; the second set include the capsules and synovial membranes of the oblique processes, the infra-spinous or yellow ligaments, the inter-spinous, the supra-spinous, and the inter-transverse. The bodies of the vertebræ are united by an anterior, a posterior, and an intervertebral ligament.
The anterior vertebral ligament (pl. 124, fig. 42) is a strong band of fibres extending from the atlas to the sacrum along the anterior face of the spine, and adhering strongly to the bones, particularly to their edges and to the intervertebral substances. Its object is to attach the vertebræ together, to strengthen the intervertebral ligaments, and to oppose excessive extension of the column.
The posterior vertebral ligament (pl. 124, fig. 74), in part a prolongation of the apparatus ligamentosus, extends down the back part of the bodies of the vertebræ, along the front of the spinal canal. It adheres more closely to the edges of the vertebræ and to the intervertebral ligaments than to the middle of each vertebra, and runs out in the sacral canal. Its object is to give strength to the spine by opposing too much flexion of the column.
The intervertebral ligaments (fig. 101,2) are placed between the bodies of all the vertebræ except of the first and second. They are fibro-cartilages, partaking both of cartilage and ligament in their character. Their union above and below to the flat surfaces of the vertebræ is so intimate, that maceration or boiling alone can separate them completely; and their own strength and cohesion surpass that of even the bones themselves, the bone breaking before the ligament can be ruptured or torn from its attachment. In the neck and loins they are thicker in front than behind, the contrary being the case in the back; this causes much of the peculiar curvature of the spine.
The oblique or articulating processes of the vertebræ are connected by synovial membranes and by ligamentous capsules extending irregularly around these so as to form imperfect capsular ligaments.
The ligamenta subflava (fig. 111) are situated between the back parts of the plates or the arches of the vertebræ; they close the intervals between them, and thus complete the back part of the spinal canal. The name is derived from their yellow color. The supra-spinous ligament (fig. 121) extends in the median line from the occiput to the sacrum, connecting the extremities of the spinous processes. The cervical portion is usually considered as a distinct portion under the name of ligamentum nuchæ, attached above to the occipital bone, below to the last cervical spine, and intermediately by distinct slips to all the cervical spines except that of the atlas. The inter spinous ligaments (fig. 122) are fibrous membranes placed vertically, and filling the space between the spinous process. The inter-transverse ligaments are ligamentous fibres extending between the transverse processes.
Special Anatomy of the Thorax
Bones of the Thorax
The thorax is constituted posteriorly by the twelve dorsal vertebræ, laterally by the twelve pairs of ribs, and anteriorly by the costal cartilages and sternum.
The sternum or breast bone (pl. 122, fig. 3, h) is situated in the anterior portion of the thorax, in its median line. The anterior surface is flat or slightly convex, and is marked by transverse lines which indicate an original division into six pieces. Of these lines the two uppermost are most prominent. The posterior surface is smooth and slightly concave. The superior or cervical end is thick and broad, and very concave transversely. In the adult, it consists of three distinct divisions, the upper of which, having attached to it the clavicle and the first and half of the second rib, is known as the manubrium. The middle piece, or gladiolus, presents six notches on each side: The inferior extremity is known as the xiphoid process: this is thin and cartilaginous, expanded towards the extremity, where it is rounded, pointed, or bifid. There is frequently a perforation in the centre.
The ribs, costæ (pl. 122, figs. 3, 4, and 5), are twelve in number on each side. They extend in an arched manner from the vertebræ towards the sternum, to which the seven superior pairs are attached by separate cartilages. These are the true or vertebra-sternal ribs. The five inferior pairs do not reach the sternum, but are connected anteriorly with each other and to the cartilages of the last true rib; they are known as false or vertebro-costal or asternal ribs. The two last pairs are sometimes called floating or vertebral ribs. The length of the ribs gradually increases from the first to the eighth pairs, then diminishes again to the last. The external surface of the body is smooth and convex; the internal is concave. The upper border is round and smooth, and gives attachment to the intercostal muscles. The inferior border is thin and marked with a groove on the inner side; its edges give attachment to the intercostal muscles, while in the groove are lodged the intercostal vessels.
The posterior end of a rib presents a head, neck, and tuberosity. The head is round and divided by a ridge into two articular surfaces, the inferior of which is the larger; these are received into the depressions in the dorsal vertebræ: an interarticular ligament is attached to the middle ridge. The head is supported by the neck, which lies in front of the transverse process, to which its posterior surface is connected by a ligament. Beyond or external to the neck is the tubercle, which looks backwards and downwards, and is divided into two portions. Of these, the internal is smooth for articulation with the transverse process of the inferior of the two vertebræ, to whose bodies the head of the rib is connected. The external is rough for the insertion of a ligament.
The cartilages which connect the ribs with the sternum must be considered as part of the skeleton. They are twelve in number on each side, and of nearly the same form as the shafts of the ribs. They serve to give great strength and elasticity to the thorax, and permit the free play required by the lungs and heart.
Articulations and Ligaments of the Thorax
The head of each rib is secured to the vertebræ by an anterior or stellate ligament, an interarticular, and two synovial membranes. The tubercle is secured in its socket by a synovial membrane, and by an external posterior and an anterior or internal costo-transverse ligament.
The capsular, stellate, or anterior ligament (pl. 125, fig. 12) arises from the front of the head of the rib, and thence extends over the two synovial membranes in a radiated manner, and is inserted by three bands, one into the sides of the vertebræ above and below, and the third into the intervertebral substance. The interarticular ligament (fig. 13) arises from the projecting ridge on the articular surface of the rib, and is inserted into the cavity in the intervertebral substance into which the head is received; it separates the two synovial membranes.
In respect to the attachments of the tubercle, the external or posterior costo-transverse ligament (pl. 125, fig. 22) arises from the posterior surface of the extremity of the transverse process; passes outwards and is inserted into the rough, non-articular portion of the tubercle of the corresponding rib. It exists on all the ribs. The middle costo-transverse ligament (fig. 23) connects the back part of the rib with the front of the corresponding transverse process. The anterior or internal costo-transverse ligament (fig. 24), wanting in the first and twelfth ribs, arises from the lower border of the transverse process, and is inserted into the crest on the upper edge of the rib beneath.
The cartilages of the ribs at their costal ends are convex, and are very closely united to the concave surfaces in the extremities of the bones by a sort of gomphosis. The articular ends of the cartilages are attached to the sternum by radiating ligaments, known as anterior, posterior, superior, and inferior sterno-costal (pl. 124, fig. 142, and pl. 125, fig. 3).
Special Anatomy of the Superior Extremities
Bones of the Superior Extremities

Each superior extremity consists of the shoulder, arm, forearm, wrist, and hand: the whole limb comprises thirty-two bones, the sesamoid not included. The shoulder is composed of the clavicle and scapula; the arm, of the humerus; the forearm, of the radius and ulna; the carpus, or wrist, of the eight small carpal bones; and the hand, of five metacarpal and fourteen phalangeal bones.
The clavicle, or collar bone (pl. 122, fig. 31), is a long bone extending from the summit of the sternum obliquely across the first rib, upwards, backwards, and outwards to the acromion process of the scapula. It is curved like an italic f, and presents two extremities and a body or shaft. The sternal end is a thick, triangular, articulating surface, with the circumference roughened for the attachment of ligaments. The body is rounded in the middle and flattened towards the extremities. The acromial end is rough above and below, and at its termination presents a small articulating surface for the acromion scapulas. The clavicle serves to support the scapula, and to prevent it from falling too far forwards or inwards; it serves as a fixed point for certain muscles, and it protects the vessels and nerves of the upper extremity.
The scapula, or shoulder blade (figs. 42, 10, 11, 12), is situated at the upper, lateral, and posterior part of the chest, and extends from the second to the seventh rib. It is irregularly flat and triangular, presenting an internal and external surface, three edges, and three angles. The internal or anterior surface (fig. 11) is slightly concave, and divided by three or four prominent lines into several broad grooves filled by the fasciculi of the subscapular muscle. Above and below these is a smooth flat surface for the attachment of the serratus magnus. The external or posterior surface or dorsum (pl. 122, fig. 10) is convex, and divided into two unequal parts by a ridge or spine (fig. 102). This spine, arising gradually from the margin of the scapula, increases in height as it proceeds forward, and becoming flattened above and below. It terminates in an eminence named the acromion process (fig. 103). The external surface of this process is roughened, while near the apex is seen the articulation with the clavicle. Above the spine is the supra-spinatus fossa, filled by the supra-spinous muscle. The infra-spinatus fossa, below the spine, is larger. In the superior border or costa of the scapula is seen a notch, the supra-scapular (fig. 106), converted into a foramen by ligaments; through this passes the supra-scapular nerve. From the anterior part of this border, in front of the notch, there arises the coracoid process (figs. 105, 113); this overhangs the upper and inner part of the glenoid cavity. The base of the scapula, or the posterior border, is the longest margin of the bone. The anterior, inferior, external, or axillary costa (fig. 121) leads from the glenoid cavity, this being situated at the convergence of the two costæ. The glenoid cavity (fig. 122) is supported on a contracted neck; it consists of a shallow concavity, in which plays the head of the humerus. In life or the fresh subject, this cavity is deepened by the fibrous glenoid ligament.
The arm is composed solely of the humerus or brachium (pl. 122, fig. 3 c). It is the longest and largest bone in the upper extremity, and presents a body or shaft, with two extremities. The upper or scapular extremity is the larger, and consists of the head, neck, and two tubercles. The head (fig. 13) is hemispherical, inclined upwards, inwards, and backwards; it is smooth, and covered with cartilage for articulating with the glenoid cavity of the scapula. The neck is the slightly contracted line or furrow round the head; it is roughened for the attachment of the capsular ligament. The tuberosities are two, the greater (fig. 34) and the lesser (fig. 35). Between these tubercles is the deep groove for the long tendon of the biceps muscle. The body or shaft of the humerus is thick and round above, twisted in the middle, expanded and somewhat triangular below. The lower extremity of the humerus (fig. 14) is flattened, elongated transversely, and twisted a little forwards. It presents internally the internal condyle (fig. 36), which is very prominent; externally is the external condyle (fig. 37), not so prominent as the internal, and situated lower down. Between and below these condyles is a series of articulating eminences and depressions, partly turned forwards: they consist externally of a small round head of the radius, internal to which is a slight depression, corresponding to the margin of the radius. Internal to this is a sharp semicircular ridge, extending round the lower end of the bone, separating the radius and ulna. Next comes the trochlea, for articulation with the ulna. At the anterior extremity of this trochlea is a depression for the reception of the coronoid process, and at the posterior is another, for receiving the olecranon process of the ulna. The bone between these two depressions is thin and transparent, and sometimes deficient by absorption.
The forearm (pl. 122, fig. 3, d) is composed of the ulna and radius. Of these, the ulna or cubitus (figs. 39, 151) is situated at the inner side of the forearm, forming the principal part of the elbow; it does not directly enter into the wrist joint, but falls a little short of it below; it is divided into the body and two extremities. The upper extremity is the larger, and presents two processes and an intervening cavity. The posterior process, or the olecranon (figs. 16, 17, and 18), is the highest part of the bone: posteriorly it is smooth; anteriorly it is also smooth, and covered with cartilage. The coronoid process (fig. 172) is anterior and inferior to the preceding. Externally it is hollowed out into the lesser sigmoid cavity (fig. 173) which receives the head of the radius; superiorly it leads into the great sigmoid cavity (fig. 161) which moves on the trochlea of the humerus in flexion and extension of the forearm; the profile of this cavity resembles the letter C. The lower or carpal end (fig. 211,2) is small and round, with two eminences. The external is named the head; it is round, and covered with cartilage, and received into the cavity in the inner border of the radius. The internal eminence, or styloid process (fig. 212), is more prominent, and on a level with the posterior surface of the bone. The ulna articulates above with the humerus and radius, and below with the radius and interarticular cartilage.
The radius (figs. 38, 152) is shorter than the ulna, and, while only accessory as a rotating bone in the elbow, it is the principal bone in the carpal joint. It is divided into the body and two extremities. The upper or humeral end presents a head, neck, and tubercle. The head (fig. 191) is a circular superficial cavity, with the surface and circumference covered with cartilage, the former to articulate with the small head of the humerus, the latter with the sigmoid cavity of the ulna and with the annular ligament. The neck (fig. 192) is nearly an inch long, descends obliquely inwards, and is contracted and circular. At its lower extremity, where it joins the shaft, is the tubercle (fig. 193). The body or shaft is somewhat triangular, and presents three surfaces, separated by three margins or angles. The lower or carpal end of the radius is irregularly square; its anterior prominent edge gives attachment to the anterior carpal ligament. Posteriorly there are seen three grooves: one nearly in the middle line, the second at the ulnar side of this, and the third on the radial side. The styloid process is the inferior extremity of the radius; from its point arises the external lateral ligament of the wrist.
The hand (pl. 122, fig. 3 e; pl. 123, figs. 46 and 47) consists of the carpus, metacarpus, and phalanges; twenty-seven bones in all.
The carpus is composed of eight bones, arranged in two rows: the first row consists of the scaphoid, lunar, cuneiform, and pisiform; the second of the trapezium, trapezoid, magnum, and unciforme; enumerating them from the radial to the ulnar side, or from without inwards.
The scaphoides or navicular bone (pl. 123, fig. 471). This is the largest in the upper row, and is situated at its outer or radial side. It presents four articular surfaces, by which it articulates with the radius, the trapezium, the trapezoid, the lunar, and the magnum. The lunare or semicircular bone (pl. 123, fig. 472) is smaller than the scaphoid. It also has four articular surfaces, for articulation with the radius, the os magnum, unciforme, scaphoides, and cuneiforme. The cuneiforme or pyramidal hone (fig. 473) is wedge-shaped, with the base looking outwards, and articulating with the lunare. Its other articulations are to the unciforme and pisiforme. The pisiforme is pea-shaped, and the smallest bone in the carpus, at the upper and inner part of which it is placed. It articulates with the cuneiforme by a small circular surface. The trapezium (fig. 475) is the most external of the second row of the carpus; it meets the scaphoid, the trapezoid, and the first and second metacarpal bones. The trapezoides (fig. 476) is less in size than the latter; it articulates with the scaphoid, the trapezium, the magnum, and the second metacarpal. The os magnum (fig. 478) is the largest bone in the wrist. It supports the second, third, and fourth metacarpal bones, and joins the scaphoid, the lunar, the trapezoid, and the unciform bones. The unciform bone (fig. 478) is next in size to the magnum. Situated at the lower and inner part of the carpus, it articulates with the fourth and fifth metacarpal bones; also with the lunar, the magnum, and the cuneiform.
The metacarpal hones belong to the class of long bones. They are five in number (fig. 462), and are nearly parallel with each other. All are concave on the palmar surface, convex on the dorsal, and large at each extremity. The posterior or carpal end is of rather irregular figure; the anterior presents a round head. They are articulated anteriorly with the bases of the first phalanges, and are flattened at the sides for the attachment of ligaments.
The fingers are composed each of three phalanges, except the thumb, which has but two. The first, or those nearest the carpus, are largest; next come the middle; the third row being the smallest. The posterior convex surface of the last, or ungual phalanx, supports the nail. On the fore part of the articulation between the metacarpal bones and the first phalanx of the thumb, there are generally two small sesamoid bones. These, with their analogues occurring in various situations in the body, do not properly belong to the osseous system, being rather accessories to the tendons of muscles.
Articulations and Ligaments of the Superior Extremities
The ligaments of the superior extremities comprise, 1. Those which connect the clavicle with the sternum; 2. Those connecting the clavicle with the scapula; 3. Those proper to the scapula; 4. Those connecting the humerus with the scapula; 5. Those connecting the bones of the elbow joint; 6. Those of the wrist joint with those of the inferior radio-ulnar; 7. Those of the metacarpus; 8. Those of the phalanges of the fingers; 9. Those connecting the metacarpus and the phalanges.
1. Sterno-clavicular Articulation. This articulation (pl. 125, figs. 8, 9, 19) is arthrodial, and is secured by an anterior, posterior, inferior, and inter-clavicular ligament, as also by an inter-articular cartilage and two synovial membranes.
The anterior sterno-clavicular ligament arises from the end of the clavicle, descends inwards, and is inserted into the fore part of the sternum. The posterior ligament takes a course behind the joint, parallel to the preceding, and adheres to the joint, restin r upon the sterno-hyoid muscle. These two ligaments (pl. 125, fig. 81, fig. 91) are so expanded over the joint as to resemble a capsular or orbicular ligament.
The inferior costo-clavicular or rhomboid ligament (fig. 95) passes from the lower surface of the sternal end of the clavicle downwards, forwards, and inwards, and is inserted into the cartilage of the first rib; it closes the angle between it and the clavicle.
The inter-clavicular ligament (fig. 82, fig. 92) extends from the posterior surface of one clavicle to the other; its lower border is generally attached to the posterior lip of the sternum. Its office is to connect the clavicles with each other and with the sternum. The inter-articular cartilage (fig. 94) is nearly circular, very thin, and often perforated in the centre. On each side is a dry synovial membrane.
2. Scapulo-clavicular Articulation. The oval end of the clavicle is connected with that of the acromion process by a plain arthrodial joint, which is secured by a superior and an inferior acromio-clavicular ligament (fig. 101). These are attached to the surfaces of each bone, and being united or continuous both before and behind, the joint may be considered as a strong orbicular ligament. The coraco-acromial ligament really consists of two, the conoid (fig. 102) and the trapezoid (fig. 103). The former is posterior and the smaller of the two; and while united posteriorly and externally, anteriorly they are very distinct.
3. Proper Ligaments of the Scapula. These are two in number, an anterior and a posterior. The anterior, deltoid, or coraco-acromial ligament (fig. 104) arises from the coracoid process, passes upwards, and is inserted into the point of the acromial process. The posterior or coracoid ligament arises from the superior costa of the scapula behind the notch, passes forwards, and is inserted into the base of the coracoid process; it converts the notch into a foramen. When this ligament is wanting, as is sometimes the case, the notch is completed into a hole by bone.
4. Humero-scapular or Shoulder Articulation. This joint is a ball and socket (enarthrodia), with the head of the humerus retained in the glenoid cavity by the capsular, the coraco-humeral or accessory, and the glenoid ligaments, and a synovial membrane.
The glenoid ligament adheres to the margin of the glenoid cavity, and deepens the socket for the head of the humerus: it is partly continuous with or derived from the long tendon of the biceps muscle. The capsular ligament (fig. 107) arises around the head of the scapula, and increasing in size, encircles the head of the humerus, and is inserted into its neck and prolonged on the periosteum. It derives great strength from the tendons of the four capsular muscles which cover and are identified with it. The coraco-humeral or accessory ligament extends obliquely downwards and outwards from the coracoid process to the anterior part of the great tuberosity. The synovial membrane is reflected over the glenoid surface around the glenoid ligament.
5. Humero-cubital Articulation, or the Elbow Joint. In this, one of the most perfect of the ginglymoid or hinge joints, the opposed extremities of the humerus, ulna, and radius mutually receive each other, and are attached together by an external and internal lateral, and by an anterior and posterior ligament. There is no distinct capsular ligament, although the aggregate of these may be considered as such.
The external lateral ligament (pl. 128, fig. 82) arises from the external condyle, and is inserted into the posterior and external part of the annular ligament of the radius. This ligament is confounded with the tendons of certain muscles. The internal lateral ligament (pl. 125, fig. 151) arises from the inner condyle, and is inserted in a radiated manner into the inner margin of the great sigmoid cavity of the ulna, between the coronoid and olecranon processes. It adheres to the synovial membrane, and, with the other lateral ligament, strengthens the articulation.
The anterior ligament (fig. 121) consists of thin fibres arising chiefly from above the internal condyle and the coronoid depression on the fore part of the humerus. Some are inserted into the annular ligament of the radius, others into the coronoid process, while the remainder are lost on the synovial membrane. The fibres of the posterior ligament extend chiefly in a transverse direction from one condyle and one lateral ligament to the other.
The articulations between the radius and ulna are two in number, one superior, another inferior. The shafts of the two bones are also connected by the interosseous ligament (fig. 161). In the superior articulation the head of the radius is received into the lesser sigmoid cavity of the ulna, and is retained in it by the following ligament.
The annular ligament (figs. 162, 172) forms about three fourths of a circle, the lesser sigmoid depression completing it. It arises from the anterior, and is inserted into the posterior border of the lesser sigmoid cavity of the ulna. It is lined by the synovial membrane of the joint; it encircles the head and neck of the radius in the same manner as the transverse ligament of the atlas confines the odontoid process of the axis.
The oblique ligament arises from the root of the coronoid process of the ulna, and is inserted into the inner side of the radius below its tubercle.
In the inferior radio-ulnar articulation, the round head of the ulna is received into the sigmoid cavity of the radius, and retained in it by a loose synovial membrane or the sacciform ligament (pl. 126, fig. 11), which is covered before and behind by some ligamentous fibres, forming an imperfect capsule, and passing from the radius to the ulna. The opposed edges of the shafts of both radius and ulna are connected by a thin aponeurosis called the interosseous membrane or ligament (pl. 125, fig. 161, 2). It is not made very tense in any position of the limb, and serves to give attachment to muscles.
6. Radio-carpal Articulations, or the Wrist Joint. In this joint, which is of great transverse extent, the lower end of the radius and the inter-articular cartilage form a socket for the scaphoid, lunar, and cuneiform bones: the two former are received into the radius; the latter corresponds to the fibro-cartilage which separates it from the ulna, and excludes this bone from the joint. The wrist joint is secured by an external and internal lateral, by a posterior and anterior ligament, and by a synovial membrane.
The external lateral or radio-carpal ligament arises from the styloid process of the radius, and is inserted into the scaphoid bone. The internal lateral or ulno-carpal ligament arises from the styloid process of the ulna, extends obliquely downwards and forwards, and is inserted into the cuneiform and pisiform bones. The anterior and posterior ligaments descend from the radius and interarticular cartilage anteriorly and posteriorly, and are inserted into the superior row of the carpus. These two ligaments, with the two lateral, constitute the capsular ligament of some authors (pl. 126, figs. 12, 3, 4, 21, 2, 3).
7. Articulations of the Bones of the Carpus. The bones of the carpus are arranged in two rows, between which a certain degree of motion takes place, very little, however, between the individual bones in either row. The bones of the first row are connected by interosseous ligaments, consisting of dense tissue placed between the upper border of the scaphoid and lunar, and lunar and cuneiform. They range on a level with the carpal convexity of the bones. The dorsal and palmar ligaments consist of strong bands, which run in different directions from one bone to another. The four bones of the second row of the carpus, like those of the first, are connected by interosseous substance and by dorsal and palmar bands. The bones of the entire carpus are connected with each other by the annular ligament which preserves the arched form of the carpus.
8. Articulations between the Carpus and Metacarpus. The five metacarpal bones present two series of articulations, the posterior or carpo-metacarpal, and the anterior or metacarpo-phalangeal. In the former, the carpal ends of the four internal metacarpal are joined to the lower row of the carpus by nearly plane surfaces, and are secured before and behind by transverse and oblique fibrous bands, which cover the synovial membranes and are called dorsal, palmar, and interosseous. Across the upper and lower extremities of the metacarpus pass ligaments (fig. 18, 9), whose object is to give compactness to the hand.
9. Articulations between the Metacarpus and the Phalanges. These joints are furnished with capsular ligaments and synovial membranes (figs. 3, 4, 5) There are also strong lateral ligaments.
Special Anatomy of the Inferior Extremities
Bones of the Inferior Extremities
To the lower extremities belong the pelvis, the thigh, the leg, and the foot, subdivided into the tarsus, metatarsus, and phalanges. The pelvis consists of four bones, the ossa innominata, the sacrum, a bone of the spine, and the coccyx; the thigh of one, the femur; the leg of three, the patella, the tibia, and the fibula; the tarsus of seven, the astragalus, the calcaneum, cuboid, scaphoid, and three cuneiform; the metatarsus of five, and the toes. of fourteen: thirty-two bones in all.
1. The Pelvis (pl. 122, fig. 3, k k, pl. 123, figs. 43, 45) is the irregular, circular shaped, bony ring at the lower end of the trunk, formed by the sacrum and coccyx posteriorly, and by the ossa innominata laterally and anteriorly; it contains some of the abdominal viscera and many of the urinary and generative organs; it also supports the spinal column above, and transmits the weight to the thigh bones, on which it rests below. The sacrum and coccyx have already been described. As each os innominatum (pl. 122, fig. 3, k) is divisible in early life into three bones, the ilium, ischium, and pubes, uniting to form the socket for the head of the thigh bone, we shall first consider these separately, and then as united into one bone, as in the adult.
a. The individual hones of the Pelvis. The os ilium (pl. 123, fig. 435) is situated at the upper and outer part of the pelvis, and forms that projection commonly called the hip. It is broad, flat, and triangular, the base above bounded by a semicircular crest, which ends before and behind in processes or tubercles named spinous; the apex below forming the upper and outer part of the acetabulum or socket; it maybe divided into the. body, ala, and processes. The body is the inferior narrowed portion; the ala is the broad, fan-like, semicircular portion which ascends from the body, inclining outwards and a little forwards; the external surface, or dorsum, is rough and irregularly convex and concave, with a considerable concavity above the acetabulum (external ilia fossa) and two curved semicircular lines, a superior and an inferior. The internal surface of the ala is divided into three parts: one, superior and anterior, is the iliac fossa; the second forms about the posterior third of the bone; and the third is smooth and small, and is the only portion of the ilium that enters into the side of the true pelvis. It is separated from the iliac fossa by a rounded edge (called the ilio-pectineal line), continuous behind with the promontory of the sacrum, and before with a sharper ridge on the pubes. The processes of the ilium are, first, the crest (pl. 123, fig. 436), forming the upper border of the ala; second, the anterior superior spine, at the anterior extremity of this crest; there is a notch between this and the third process, the anterior, inferior spine. Internal to this space is a superficial groove, bounded internally by the ilio-pectineal eminence, which is common to and formed by the union of the ilium and pubes. Fourth, the posterior superior spine is the posterior termination of the crest; and separated from this by a notch is the, fifth process, the posterior inferior spine.
The ischium (pl. 122, fig. 47, 8) is placed, at the lower, outer, and back part of the pelvis, and presents a body and processes. The body forms the outer, lower, and back portion of the acetabulum, constituting more than two fifths of it. The processes are, first, the spine (fig. 47), arising from near the middle of the posterior part, below the sacro-sciatic notch. Between this and the second process is the pulley round which the tendon of the obturator muscle turns. This next process is the tuberosity or tuber ischii (fig. 48). On this rough and broad process the body rests when in a sitting posture. Between the spine and the tuberosity is the lesser sciatic notch, converted into a foramen by the great sciatic ligament. The third process is the ramus, ascending from the tuber forwards and inwards, and joining the descending ramus of the pubes.
The os pubis (pl. 112, fig. 53) is situated at the anterior part of the pelvis, and is smaller than the ilium or ischium. It may be divided into the body and processes. The body is the most external portion, and constitutes the internal and superior part of the acetabulum. From the body the first process, the horizontal ramus, proceeds forwards and outwards, grooved beneath where it bounds the obturator foramen. At the internal extremity of this ramus is the second process, the tuberosity or spine. This is a prominent tubercle, into which Poupart’s ligament is inserted. The third process, the crest, leads transversely inwards from this spine, and at its internal end is the fourth process, the symphysis. From the lower end of the symphysis descends the fifth process, the inferior or descending ramus; this, with the ramus of the opposite pubes, forms the arch of the pubes; the outer edge of the ramus assists in bounding the thyroid hole.
b. The Pelvis as a whole. Considering in the next place the pelvis as a whole, we commence with the acetabulum (pl. 123, fig. 437), constituted by the junction of the bodies of the three bones. It is surrounded by a prominent border with a deep notch or deficiency internally, and two others of less extent, inferiorly and superiorly. The great notch which is opposite the thyroid foramen, between the ischium and pubes, is converted into a foramen by a ligament passing between these two bones. The cotyloid cavity (fig. 452) in the acetabulum for the reception of the head of the thigh bone, is of a hemispherical form, and about two inches and a half in diameter.
The obturator, or thyroid foramen, is situated at the inner side of the acetabulum and at an inferior level, and is the large anterior hole in the pelvis bounded by the ischium and pubes.
The superior circumference or base of the pelvis is formed on each side by the crest of the ilium; posteriorly by the promontory of the sacrum, anteriorly by the iliac spines, ilio-pubal eminences, the intervening grooves, and the crests and symphysis of the pubic bones. The lower or perineal circumference (strait, or outlet, of the pelvis) is directed downwards and a little forwards; bounded by the rami of the pubes,. the rami and tuberosities of the ischium, the coccyx, and in the recent state by the sacro-sciatic ligament of each side. When, as in the artificial skeleton, the latter are removed, this strait presents three notches: first, the arch of the pubes, triangular and placed beneath the symphysis; second and third, the sacro-sciatic notches between the sacrum and os innominatum of each side. Each of these is divided into a superior and an inferior by the sciatic ligaments.
The internal surface of the pelvis is divided into two parts by the ilio-pectineal line. The upper of these parts, properly part of the abdomen, is known as the false pelvis, the inferior being the true. The latter is a sort of curved canal, wider about the centre than at either end; with smooth walls, concave posteriorly from above downwards, concave anteriorly in the transverse direction, and on either side nearly plane.
The female pelvis (pl. 123, fig. 45) differs from that of the male (fig. 43) in several particulars: it is wider and larger, but not so deep; the alæ of the ilium are more expanded, the prominence of the sacrum is less, the inlet and outlet are rounder and wider, the sacrum is broader and more concave, the pubic arch more round and open, the symphysis pubis not so deep, the obturator holes are smaller and more triangular, the sciatic tuberosities are directed more outwards, and the acetabula are more distant from each other; all the bones are more thin and delicate. The male pelvis is deeper, narrower, and the bones more solid and strong. The peculiarities in the female pelvis are intimately connected with the functions of parturition.
2. The Thigh. This is constituted by but one bone, the femur (pl. 122, fig. 3 l). This is the longest and strongest bone in the skeleton, and is proportionally longer in man than in any other animal; from the pelvis it is directed obliquely downwards and inwards, this obliquity being greater in the female than in the male. It consists of the body or shaft, and two extremities.
The body is slightly twisted, very broad below, and with a rough projecting ridge down the posterior face called the linea aspera (fig. 411). This divides into two ridges at either end, and above its middle may be seen one or two holes entering obliquely upwards for transmitting the nutritive vessels of the bone.
The upper or pelvic extremity of the femur presents three eminences, the head for articulating with the cotyloid cavity, and the trochanters for the insertion of muscles.
The head (figs. 318, 24) is of a globular figure, and forms a considerable segment of a sphere; it is directed upwards, inwards, and a little forwards; a little below its centre there is a rough oval depression for the insertion of the round or articular ligament. Excepting this depression, the head is covered throughout with cartilage; it is supported by a strong elongated process of a pyramidal form, the neck (fig. 24), which forms an angle more or less obtuse with the shaft of the bone. A rough irregular line separates the head from the neck, beyond which the articular cartilage of the foramen does not extend. The great trochanter (fig. 319) is continuous with the external side of the shaft, and nearly in a line with its axis. It is thick, rough, and square; broad and convex externally. Internally it presents a pit, or digital cavity, which receives the tendons of the external rotators of the limb. The lesser trochanter (fig. 321) is a conical tubercle at the posterior and inner side of the shaft, much below the level of the great trochanter and of the base of the neck.
The inferior or tibial end of the femur (fig. 25) is very large and broad, flattened before and behind, and divided into two eminences or condyles, which are separated posteriorly by a deep notch. The condyles articulate with the tibia. The external (figs. 324, 414) is larger, and pro jects more forward than the internal; its articulating surface also is broader and ascends higher. An external tuberosity gives attachment to the external lateral ligaments of the knee-joint. Beneath it is a groove which receives the tendon of the poplitaeus muscle when the joint is flexed. The internal condyle (pl. 122, figs. 323, 413) is narrower, less prominent before, but more prolonged behind. On its inner side is the tubercle for the attachment of the internal lateral ligament. The posterior crucial ligament is attached to the rough outer side. Posteriorly the condyles are separated by a deep fossa or intercondyloid notch which lodges the crucial ligaments. Anteriorly they unite in a trochlea or pulley on which the patella moves. The femur thus articulates superiorly with the pelvis, anteriorly with the patella, and inferiorly with the tibia.
3. The Leg. The bones of the leg are the patella, tibia, and fibula.
The patella, rotula, or knee-pan (figs. 322, 54, 22, 23) is a small bone in front of the knee-joint, triangular or heart-shaped, the base above, the apex below. The anterior surface is convex and rough, the posterior covered by cartilage and divided by a vertical ridge into two parts. The patella slides in the trochlea of the femur; to the upper end the extensor tendons are attached, while the lower is connected with the tibia by a powerful ligament.
The tibia, or shinbone (fig. 3, m), next to the femur, is the longest bone in the skeleton. It occupies the anterior and inner part of the leg; the direction, unlike that of the femur, is vertical, and the tibiæ of the opposite sides are parallel. The upper extremity is thick, and expanded from side to side; the circumference somewhat circular or oval, convex in front and on the sides, but slightly grooved behind. The upper or femoral surface (fig. 26) presents two condyles, or rather glenoid cavities, for articulating with the femur. The internal is oval, and the deeper of the two; it is also larger antero-posteriorly. The external is nearly circular, and very superficial. The two are separated by a spine, which is of a pyramidal form, and is surmounted by two tubercles; in and about the spine are inserted the semi-lunar cartilages and the crucial ligaments.
The body or shaft of the tibia is triangular; its size diminishes from the head for about two thirds down; it then increases somewhat towards the lower end.
The lower or tarsal end (fig. 27) is somewhat square, with an anterior convex edge, covered by extensor tendons; a posterior nearly smooth edge, traversed by a groove; externally a concave triangular surface, smooth below for receiving the lower end of the fibula; internally there is a thick flattened perpendicular process, called the internal malleolus oy ankle (fig. 417).
The fibula (fig. 325,27) is very slender, and nearly as long as the tibia; it is placed at the outer side of the leg, nearly vertical, with its lower end inclined a little forwards; the superior or femoral end is small and circular, with a slight cavity forwards, upwards, and inwards, for articulating with the tuberosity on the external condyle of the tibia; the lower or tarsal end is larger than the upper; it is elongated into a long oval process, the external malleolus or ankle (fig. 418); the external lateral ligament arises from the point of this process.
4. The Foot is composed of twenty-six bones, which are arranged in three parts, the tarsus, metatarsus, and toes. The bones of the tarsus (pl. 122, figs. 28, 29, 330; pl. 123, figs. 48 and 49) are seven: astragalus, calcaneum, navicular, cuboid, and three cuneiform (internal, middle, and external). These are arranged in two rows, the first embracing the astragalus, OS calcis, or calcaneum; the second row consists of five bones: the cuboid bone forms it externally alone, but on the inner side it presents two short transverse rows, the navicular forming the posterior, and the three cuneiform bones the anterior.
The astragalus (pl. 123, fig. 481) comes next to the calcaneum in point of size, and is situated at the upper and middle part of the tarsus, where it is wedged between the two malleoli; superiorly it articulates with the tibia, inferiorly with the calcaneum, anteriorly with the scaphoid, and externally with the fibula.
The calcaneum or os calcis (fig. 492) is the largest bone in the tarsus, at the lower and posterior part of which it is placed: it is elongated posteriorly into a process called the heel; its upper surface presents two articulating surfaces, the support of the astragalus; the anterior extremity presents an articular surface for the cuboid bone; the posterior extremity is roughened below, for the attachment of the tendo Achillis; the inferior surface presents two tubercles, for the attachment of muscles and ligaments: externally it is flat, and marked with two shallow grooves, separated by a spine; internally it is broad, and hollowed out into an arch, through which pass various nerves, vessels, and tendons.
The navicular or scaphoid bone (fig. 483) is situated about the middle of the tarsus, and at its upper and internal part; of an oval form, its long axis directed downwards and forwards: the posterior surface forms a superficial glenoid cavity, for the head of the astragalus; the anterior surface is convex, and divided by two vertical ridges into three surfaces, for the three cuneiform bones; on the external side there is usually a small flat articular surface, for the cuboid bone; the scaphoid is connected to the calcaneum by a strong ligament.
The cuboid bone (fig. 487) is situated at the outer and anterior part of the tarsus, external to the navicular, and anterior to the calcaneum; it articulates posteriorly with the calcaneum, internally with the scaphoid and the external cuneiform, and anteriorly with the fourth and fifth, or the two external metatarsal bones.
The three wedge-shaped cuneiform bones (fig. 484, 5, 6) are situated at the anterior part of the tarsus, between the scaphoid and the three internal metatarsal bones: the first or internal is the largest, and the middle the smallest; the first articulates with the scaphoid, the second metatarsal, and the second cuneiform; the second also articulates behind with the scaphoid, before with the second metatarsal; the third articulates anteriorly with the third metatarsal, posteriorly with the scaphoid, internally with the middle cuneiform and with the second metatarsal, and externally with the cuboid and with the fourth metatarsal.
The metatarsus (fig. 488) consists of five long bones, parallel, and separated by interosseous spaces: its posterior border is connected to the tarsus by an irregular transverse line of articulation; convex forwards, concave backwards. The first or internal of these bones is shortest and thickest; its anterior end supports the great toe. The second is the longest; its tarsal end is articulated to the three cuneiform bones. The third is a little shorter than the second; its base rests on the third cuneiform bone. The fourth is still shorter; it rests on the cuboid bone, and touches the third cuneiform. The fifth is shortest, excepting the first; it rests on the cuboid bone, with a styloid process externally for the insertion of a muscle. The heads of all the metatarsal bones are round, the bases flat and somewhat square, to articulate with the tarsus; the sides of the bases also are flat, to join one another.
The toes (pl. 123, fig. 4[8]9, 10, 11) are five in number: the first or great toe has only two phalanges; all the rest have three, making fourteen phalanges in all. The first phalanges are longest; the second are very short; the third, also, are very small. At the base of the first phalanx of the great toe there are usually two sesamoid bones, over which the small muscles of this toe glide; the sesamoid bones may also occur in some of the other toes.
Articulations and Ligaments of the Inferior Extremities
1. Articulation between the Pelvis and the Spine. The last lumbar vertebra is joined to the sacrum in the same manner as the other vertebræ are joined to each other, by an intervertebral, anterior and posterior, yellow, supra, and interspinous synovial membranes, and capsular ligaments. The connexion is also strengthened by the lumbo-sacral ligament, a short, thick, fibrous band, extending from the transverse process of the last lumbar vertebra to the posterior part of the base of the sacrum.
The two last lumbar vertebræ are connected with the ilium by the ilio-lumbar ligament (pl. 125, figs. 44, 53,4). This is sometimes divided into two; it arises from the transverse processes of the fifth and fourth lumbar vertebræ, and from the back part of the sacrum, and is inserted into the posterior superior spine of the ilium, and into its crest.
The articulations of the pelvic bones with each other are the sacro-coccygeal, the sacro-iliac, the sacro-sciatic, and the pubic. There are no perfect or true joints between the pelvic bones.
The sacrum and coccyx are joined by a thin anterior, and a thick posterior sacro-coccygean ligament (figs. 43, 52), as also by a thin intervertebral fibro-cartilage. The articulation usually allows of more motion in the female than the male.
The sacro-iliac articulation is secured by an anterior and posterior ligament. The anterior sacro-iliac ligament (fig. 46) is thin, and consists of fibres passing transversely from one bone to another; the posterior (fig. 55) consists of fasciculi passing from the rough surface of the sacrum to that of the ilium, and to its posterior superior spine. The sacro-iliac symphysis connects the articular surface of these bones, which in the aged are sometimes anchylosed.
The sacrum and ischium, though not in contact, are connected by very strong and important ligaments. The posterior or great sacro-sciatic ligament (pl. 125, fig. 56) arises from the lower and back part of the posterior inferior spine of the ilium, and from the back part of the sacrum and coccyx; it is inserted into the lower and inner edge of the tuber ischii, and by a falciform process into the ramus of the ischium. By its upper border it converts the lesser sciatic notch into a foramen, and by its lower it completes the posterior and lateral boundary of the lower opening of the pelvis on each side. The anterior or lesser sacro-sciatic ligament (fig. 57) crosses in front of the former; it arises from the side of the sacrum and coccyx, and is inserted into the spine of the ischium. It separates the two sciatic foramina.
The symphysis pubis (fig. 7) connects the vertical oval surfaces of the ossa pubis. It is covered in front by a thick fibrous tissue, called the anterior pubic ligament; the superior and posterior pubic ligaments strengthen it superiorly and posteriorly; the sub-pubic ligament is situated beneath the symphysis.
2. The Ilio-Femoral Articulation, or the Hip Joint (pl. 126, figs. 6 and 7). This is the strongest and most perfect enarthrodial, or ball and socket joint, in the system. It includes the head of the femur and the acetabulum, both of which are incrusted with cartilage, and is secured by a capsular and an accessory ligament, a synovial membrane, an inter-articular, cotyloid, and a transverse ligament.
The ilio-femoral capsular ligament arises from the os innominatum by a very strong attachment; passes downwards and upwards, incloses the cotyloid ligament, but does not adhere to it except at the notch; enlarges opposite the head of the femur, then becomes flattened and contracted to embrace the cervix, the greater part of which it incloses. Its insertions into the upper part of the femur are partly into the bone, and partly into the periosteum.
The accessory or ilio-femoral ligament is a strong fibrous band, incorporated with the capsular, arising from and around the spinous process of the ilium, and is inserted into the anterior inter-trochanter line, near the lesser trochanter.
The synovial membrane is exposed by dividing the capsular ligament, whose internal surface it lines to some extent.
The cotyloid ligament (fig. 71) is the fibro-cartilaginous lip which deepens the acetabulum, and at the same time narrows its orifice, so as to hold the head of the femur even after the capsular ligament and all the muscles have been divided; it fits so tightly around it that the head appears to be retained in the socket partly by atmospheric pressure. The transverse ligament consists of ligamentous bands, passing across the notch in the border of the acetabulum, and completing the margin of tho cavity.
The inter-articular or round ligament, ligamentum teres (fig. 73) arises by two flat bands from the margins of the cotyloid notch, runs upwards, backwards, and outwards, and is inserted into the depression on the head of the femur.
3. The Femoro-tibial Articulation, or the Knee Joint. The condyles of the femur, the head of the tibia, and the patella, enter into this articulation; the fibula is only remotely connected with it. The ligaments which secure it may be classed into those external and those internal to the synovial membrane. The external ligaments are the ligamentum patellæ, ligamentum posticum, and the internal and external lateral ligaments. The internal are the two crucial, the inter-articular fibro-cartilages, the transverse, and certain folds of the synovial membrane.
The ligamentum patllæ, (pl. 126, fig. 81,2) consists of strong, parallel, glistening, tendinous fibres which arise from the inferior angle and from the anterior surface of the patella, and are inserted into the tubercles of the tibia. This ligament is principally a continuation of the extensor tendon, in which the patella was developed first in the form of a cartilage.
The posterior ligament arises from the tendon of the semi-membranous muscle, and ascends obliquely from behind the inner condyle of the tibia to the external condyle of the femur.
The internal lateral ligament (figs. 84, 94) arises from the back part of the tuberosity on the inner condyle of the femur, below the insertion of the tendon of the abductor magnus; descends obliquely forwards, and is inserted into the internal condyle of the tibia.
The external lateral ligament (figs. 86, 97) arises from the back part of the tuberosity on the external condyle, above the fossa for the poplitaeal tendon; it is thick, round, and smooth; descending, it is inserted into the outer side of the head of the fibula.
The synovial membrane of the knee is the largest of its class in the body.
The internal ligaments in the knee joint are the alar, mucous, transverse, crucial, and semi-lunar cartilages.
The alar ligaments (fig. 83) are only folds of the synovial membrane, in some measure produced by the displacement and eversion of the patella. They are one on each side of the bone, the internal being the most distinct.
The ligamentum mucosum or adiposum (fig. 111, 2) is only a small fold or tubular process of the same membrane: of a conical form, it arises broad from the fatty substance behind the ligamentum patellae, passes backwards and upwards, and is inserted into the notch between the condyles. The transverse ligament extends between, and is attached to the anterior convex portions of the two semi-lunar cartilages above the articular fatty mass.
The crucial ligaments (fig. 105, 6) are the most important of the inter articular cartilages. They are two strong, twisted, fibrous cords, which pass from the notch in the femur to the median line of the head of the tibia. They cross each other in passing to their respective attachments, this decussation resembling the letter X, whether viewed laterally or before or behind. They serve to attach the femur to the tibia, to steady one bone on the other, and to prevent any lateral displacement.
The semi-lunar cartilages (figs. 113, 4, 107, 8) are placed upon the articular surfaces of the tibia. The convex margin of each is thick, and connected by its edges with the synovial membrane, and between these with the external ligaments and fascia. The anterior and posterior extremities of each are fibrous, and fixed to the head of the tibia by insertions known as the oblique ligaments. They serve to deepen the articular surfaces of the tibia, and thus to retain the condyles of the femur. They also lessen the effect of concussion in the joint and in the limb generally.
4. Superior Tibio-fibular Articulation. But little motion exists between the tibia and fibula at their superior extremities: the joint is, however, secured by a distinct synovial membrane, sometimes communicating with that of the knee joint; there is also a distinct anterior and posterior ligament, the former of which is the stronger.
5. Inferior Tibio-fibular Articulation. Here the inferior extremity of the fibula is convex, and received into a depression on the tibia: both surfaces are rough superiorly, and covered by cartilage inferiorly: they are connected with each other by a strong anterior and posterior ligament. The synovial membrane is only a small cul de sac continued from that of the ankle joint. Above this is the interosseous ligament, which fastens the bones very closely and firmly together. Very little motion occurs in this joint beyond a slight yielding of one surface against the other.
6. Articulation of the Ankle (pl. 126, figs. 13, 14). This is the most perfect ginglymoid or hinge joint in the body, excepting that between the ulna and humerus. A deep mortice-like cavity, with an antero-posterior edge, is formed by the lower surface of the tibia, and by the two malleoli. The fibula forms little more than the outer wall of this cavity. In this plays the trochlear surface of the astragalus. The joint is secured by very strong lateral ligaments, also by a synovial membrane and by an anterior ligament.
The internal lateral or deltoid ligament (fig. 144, 5) arises from the internal malleolus, descends in a radiated manner, and is mserted into the astragalus, navicular, and os calcis.
The external lateral ligaments are three, a posterior, middle, and anterior. They all arise from the external malleolus, and are inserted into the astragalus or os calcis (fig. 146, 7).
The anterior or tibio-tarsal ligament arises from the anterior edge of the tibia and tibio-peroneal ligament, and is inserted into the upper and outer part of the astragalus.
7. Articulation of the Bones of the Tarsus. The seven bones of the tarsus are connected in such a firm and close manner as to admit of little motion between any two except at the articulation between the astragalus and the scaphoid.
The astragalus is connected with the os calcis by a strong interosseous ligament. There are also two synovial membranes. The head of the astragalus fits into the glenoid surface of the scaphoid, in which it enjoys considerable motion. The synovial membrane in the joint is covered superiorly by the superior astragalo-scaphoid ligament. Below is the inferior calceo-scaphoid ligament (fig. 161) extending from the anterior inferior part of the os calcis to the lower surface of the scaphoid. There is another strong ligament in this joint, called the superior calceo-scaphoid. The inferior and superior calceo-cuboid ligaments (fig. 162), as their name indicates, unite the calcaneum witli the cuboid bone. The union of the scaphoid and cuboid is effected by the dorsal and plantar scapheo-cuboid ligament. The three cuneiform bones are connected to the scaphoid by dorsal ligaments, and by flat bands, as also by very strong plantar ligaments.
8. Tarso-Metataesal Articulations. The three internal metatarsal bones are joined to the three cuneiform, and the fourth and fifth metatarsal to the cuboid. The tarso-metatarsal range of articulations is secured by strong transverse ligaments, dorsal and plantar, and by interosseous fibres.
9. The Metatarso-Phalangeal Articulations are arthrodial, and furnished with synovial membranes, protected by dorsal, plantar, and lateral ligaments. The phalanges of all the toes form ginglymoid joints, and are articulated to each other by synovial membranes and by lateral ligaments like those of the fingers.
![]() The Muscles, or Myology of the Human Frame
The Muscles, or Myology of the Human Frame
 The Muscles, or Myology of the Human Frame
The Muscles, or Myology of the Human FrameGeneral Anatomy of the Muscles
The muscles consist of aggregations of parallel, soft, contractile fibres, so connected with the bony framework and other parts of the system as to produce the various motions of the body. They constitute the portion of the animal usually known as the flesh, being composed of a peculiar reddish contractile tissue (tela muscularis), together with tendons, fat, blood-vessels, and nerves.
The muscles of the body have been divided into voluntary and involuntary, or those which are and those which are not under the control of the will. With this difference another is usually conjoined, viz. that the fibres of voluntary muscle are solid organs, exhibiting transverse and very close parallel lines, while the involuntary muscular fibre is hollow and consists of flattened bands, generally of a pale color, without transverse striae, and bulged at frequent intervals by elongated corpuscles. While the former are parallel to each other, the latter are interwoven and arranged in many layers, so as to form a muscular skin, as in the intestinal canal, the bladder, &c. Their action is confined to the enlarging, contracting, or otherwise affecting the shape and size of certain cavities, and is dependent upon the influence of the sympathetic nerves. Still the division above referred to is not altogether correct, since the heart is composed of transverse fibres, while the muscular coat of the œsophagus often displays the striæ as far down as the stomach. The further consideration of the involuntary muscles will be more appropriate under the subject of Splanchnology; that of the voluntary will now occupy our attention.
The muscles of voluntary motion, then, or the flesh proper, are usually of a deep red color; they are mostly attached to the bones by means of tendons, and thus put them in motion. All, with few exceptions, have their antagonists, or muscles whose action is in a directly contrary direction; the equilibrium being maintained by the influence of the nerves, the brain, and the spinal marrow.
Considering a muscle in itself, we find that at the more fixed place of its attachment it is usually thinner than elsewhere; this portion is called the head or origin; the middle and thicker part is the belly; while the opposite attachment is the tail or insertion. These extremities are usually tendinous, either entirely or partly. Their forms vary with the motion to be effected. Radiated muscles are those in which the fibres converge to a common point from a wide base, as in the diaphragm. Sphincter muscles are circular or annular, inclosing some cavity to be shut by their contraction, as in the eyelids, the mouth, and the anus. Broad muscles are thin and wide-spread, surrounding large cavities, as in some of the abdominal muscles. They usually arise by slips or points from neighboring muscles, and are inserted by a broad skin-like tendon. In longitudinal muscles, the fibres run parallel to each other, and are either simple or compound. They are simple when they arise by a single head and are inserted into one point, and compound when there is a plurality of either heads or insertions, or of both. Some arise by numerous digitations or dentations, with one belly; others have several bellies. When there is a long tendon in the centre, to which the fibres from opposite sides converge obliquely those on the same side being nearly parallel, the muscle is said to be penniform (musculi pennati) semi-pennati, when the fibres are on one side only.
Muscles, in respect to their antagonism, bear different names, according to the precise nature of the motions effected by them. Thus we have flexors and extensors, sphincters, elevators and depressors, protractors and retractors, &c. Their nomenclature also varies with their position, direction, shape, size, combination, origin, attachment, &c.
Muscles are assisted in their operation by tendons, usually placed at the insertion, but sometimes at both origin and insertion. They may exist at either end or at both, and again may not occur at all. Tendons may present themselves under two shapes: one like a cord, varying from cylindrical to paraboloid; the other is spread out into a membrane, and resembles an aponeurosis. They are readily recognisable by their white and shining appearance, possessing no elasticity; they are lacerated sooner than they can be stretched. They are composed of desmoid tissue, the fibres of which are united by a compact cellular substance in small quantities. The fibres are longitudinal, and may readily be separated by maceration or slight boiling. In ordinary health no red blood penetrates the tendons; in inflammation, however, their capillaries may become so much enlarged as to admit red globules; no nerves have ever been traced into them. They are more soluble in boiling water than the ligaments. They have a great affinity for phosphate of lime, and hence they are frequently found hardened by the development of bony matter, especially where they run over long trochleæ. The patella is an illustration of this ossification of tendon, as also the sesamoid bones found under various circumstances. Tendons are frequently confined to a motion in one direction by passing through sheaths, or through loops, or else by the intervention of pulleys (trochleæ), in or over which they glide.
For the sake of facilitating the play of tendons, and to prevent friction, they are surrounded by loose cellular membranes (vaginæ tendinum mucosæ) which permit them to glide freely one on the other; in other places they glide over synovial sacs of a similar character (bursæ mucosæ) especially about the joints.
Anatomy of the Faciæ

The muscles are intimately connected with certain membranous expansions (fasciæ) found in various regions of the body, and forming coverings to particular parts. These expansions are composed either of cellular tissue more or less condensed, or of fibrous tissue; the former are called cellular fasciæ, the latter the aponeuroses or aponeurotic fasciæ. They include and embrace not only single muscles but entire systems, maintaining them securely in their place and relative position. The most extensively distributed cellular fascia is that layer of cellular membrane immediately adjacent to the subcutaneous cellular tissue all over the body, and in most cases so intimately connected with it as to be inseparable. This is usually known as the superficial fascia. Although this is universal, there are nevertheless certain regions where it is of more importance than in others, as in the neck and abdomen; here it constitutes a distinct membraniform expansion. The cervical fasciæ bind down the muscles, and support the vessels and glands in this region; at the lower part of the neck they serve to protect the trachea and the upper part of the thorax from the pressure of the atmosphere during respiration.
Pl. 129, fig. 1, cervical fascia, the platysma myoides supposed to be removed: 1, superficial layer; 2, temporal aponeurosis; 3, portion over the parotid gland; 4, clavicular portion; 5, continuation over the pectoralis major; 6, external jugular vein showing through the superficial layer.
Pl. 129, fig. 2 1, middle layer of the cervical fascia; 2, cut edge of the superficial layer; 3, continuation of the middle layer beneath the sterno-cleido-mastoid muscle; 4, sheath for the cervical vessels; 5, section of the sterno-cleido-mastoid; 6, portion of the fascia attached to the lower jaw, separating the parotid gland, 7, from the submaxillary, 8.
Pl. 129, fig. 3, deep-seated layer: 1, section of the superficial layer; 2, do. of the sterno-cleido-mastoid; 3, middle layer; 4, deep-seated layer extending into the thoracic cavity, and passing above along the lower edge of the thyroid gland, 5.
Pl. 129, fig. 4 1, layer descending anterior to the vertebral column; 2, scalenus anticus forming a swelling beneath it; 3, clavicle removed; 4, section of sterno-cleido-mastoid.
The eye is protected in a measure by the ocular fascia, which, although not very thick or strong, is tough, flocculent, and difficult to remove. It covers the recti muscles as far back as their origin, and is continued anteriorly over their tendons, but of a finer and denser tissue, nearly to the circumference of the cornea, and beneath the conjunctiva. It is also prolonged as a thick sheath round the trochleator tendon as far as its pulley, to which it is connected, and around the obliquus inferius to its origin. This fascia seems to connect and retain all these muscles and tendons in their proper relative situations both to each other and to the eyeball; it has, however, a still further and more interesting relation, for it is continued beneath the four recti, forming for each a perfect sheath and a non-adherent envelope for the posterior part of the eyeball.
Pl. 129, fig. 6 1, 2, aponeurotic tissue of the eyelids; 3, continuation of the same between the recti muscles, constituting a sheath to each; 4, investment of the sclerotica; 5, optic nerve.
Fig. 5 represents the axillary fasciæ.
The brachial aponeurosis invests the arm down to the elbow, over which it is partially continued into the fascia of the arm; it is weak and imperfect over the deltoid muscle, but increases in strength and tension as it descends. Its fibres are mostly in the circular direction, but many are spiral and vertical; above it is continuous with the fascia covering the pectoral and deltoid muscles; below the former it receives an addition from the fascia of the axilla (fig. 5). About the middle of the arm it adheres to the lateral ridges of the humerus by two septa named internal and external intermitscular ligaments. The brachial aponeurosis serves to confine the several muscles without restraining their actions, compressing them so as to preserve the form and symmetry of the limb; it also protects the vessels and nerves.
Fig. 18, brachial fascia: 1, portion covering the deltoid muscle; 2, portion on the arm; 3, portion on the forearm; 4, semilunar fascia of the biceps brachialis; 5, palmar fascia; 6, palmaris brevis muscle.
Fig. 19 1, carpal ligament; 2, dorsal fascia.
Fig. 7, cross section of the right arm at about the lower third of the deltoid muscle, showing the intermuscular laminæ of the brachial fascia.
Fig. 8, cross section of the right forearm at about the middle, for the same purpose.
The superficial abdominal fascia consists of a tolerably compact surface of cellular tissue and tendinous fibres, weak above but increasing in density as it descends from the thorax over the abdominal muscles. From the abdomen it extends on either side over Poupart’s ligament to the thigh, which it invests, and in the centre over the organs of generation. The superficial fascia supports and connects the fleshy and tendinous fasciculi of the abdominal muscles; it also possesses some power of resistance and a good deal of elasticity, which assists these muscles in the contraction of the parietes of the abdomen. In the lower part of the abdominal muscles is seen the abdominal ring (annulus abdominalis) placed external and superior to the pubes on each side. It transmits, in the male, the spermatic cord and the cremaster muscle, with its vessels and nerves; and in the female, the round ligament of the uterus. Its external opening pierces through the superficial abdominal fascia.
Pl. 129, fig. 11 1, rectus abdominalis; 2, superficial abdominal fascia refiexed; 3, external, and 4, internal portion of the transverse fascia; 5, posterior or inner abdominal ring.
The crural ring (annulus cruralis) is the triangular opening through which the femoral vessels emerge from the abdominal cavity. This is of a triangular form; the base externally is the femoral vein, the apex internally is Gimbernaut’s ligament; it is bounded anteriorally by Poupart’s ligament, and by the superior fibres or corner of the falciform process of the fascia lata, and posteriorly by the pubes.
Pl. 129, fig. 12 1, suspensory ligament of the penis; 2, crural ring; 3, Gimbernaut’s ligament; 4, lamina cribrosa; 5, femoral vessels.
Fig. 13 1, sheath of the femoral vessels; 2, falciform process of the fascia lata.
The iliac fascia arises from the inner border of the entire crest of the ilium, and from Poupart’s ligament external to the iliac artery. It is attached to the psoas and the iliacus muscles.
The superficial perinseal fascia occurs beneath the integument, and anterior to as well as on each side of the anus; it covers the muscles in the perinseum. The middle perinseal fascia, also called triangular ligament of the urethra, or septum perinsei, separates the anterior perinseum from the pelvis.
The pelvic fascia lines the cavity of the lesser or true pelvis.
Pl. 129, fig. 14 1, fascia of the posterior face of the obliquus externus abdominis; 2, part connected with Poupart’s ligament; 3, iliac fascia; 4, Cowper’s ligament; 5, femoral vessels.
Fig. 151, 2, superficial perinseal fascia.
Fig. 16 1, cut edge of the superficial perinaeal fascia; 2, deep-seated perinaeal fascia; 3, opening for the passage of the vessels of the penis; 4, section of the urethra.
Fig. 17 1, crural ring; 2, Gimbernaut’s ligament; 3, Cowper’s ligament; 4, iliac fascia helping to form the crural ring; 5, rectum; 6, urinary bladder laid back; 7, superficial perineal fascia; 8, opening for the perinseal vessels; 9, obturator foramen; 10, anterior ligament of the bladder.
The fascia lata is united to the spine of the ilium, to the whole length of Poupart’s ligament, as also to the linea innominata and spine of the pubes; it may be divided into three portions: the internal or pubic or pectineal, the external or iliac, and the middle or cribriform. It extends downwards over the thigh. The fascia of the leg is derived partly from the fascia lata of the thigh; it also receives additional fibres from the tendons around the knee-joint. Near the ankle it increases in strength from its connexion with the malleoli and three annular ligaments. From the anterior annular ligament a thin fascia is continued over the back of the foot; that covering the sole of the foot, or plantar fascia, is remarkably strong. Anteriorly it divides into three parts lying on different planes, and serving to separate the plantar muscles into three orders, the internal, middle, and external.
Pl. 129, fig. 20, fascia of the leg, 1, fascia covering the glutaeus maximus; 2, femoral fascia; 3, investment of the tensor vaginæ femoris muscle; 4, fascia of the leg; 5, dorsal fascia of the foot.
Pl. 129, fig. 21, cross ligament of the foot.
Fig. 22, plantar aponeurosis.
Fig. 9, cross section of the right thigh, about the middle, to show the arrangement of the fascia.
Fig. 10, cross section of the leg.
Special Anatomy of the Muscles




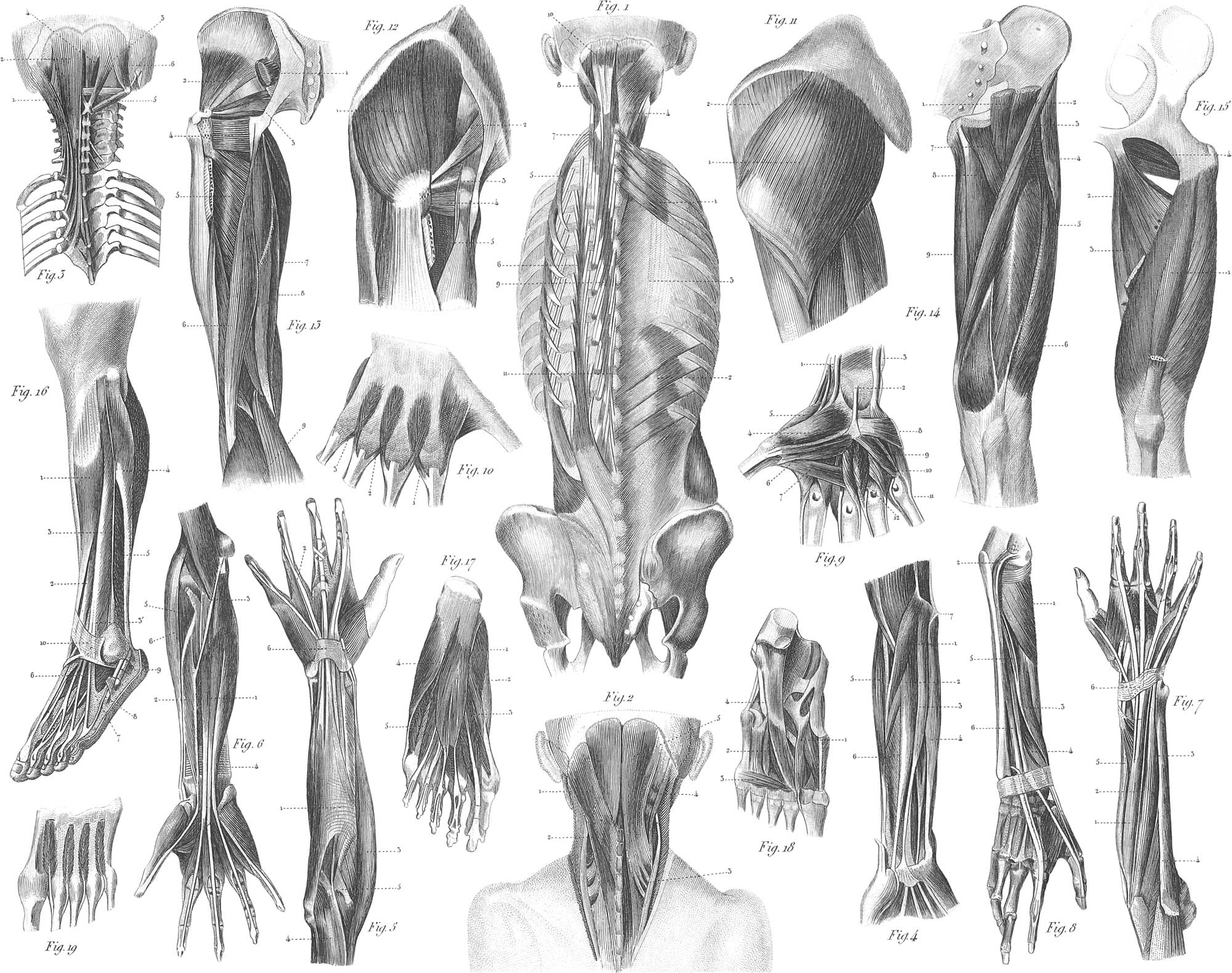
Muscles of the Head
We may divide the muscles of the head into those of the cranium and those of the face. The proper muscles of the cranium are the occipito-frontalis and the three common muscles of the ear. The superficial muscles of the face are thirty-three in number, arranged in sixteen pairs and one azygos. They belong as follows:
Three pairs belong to the palpebral; viz. orbicularis palpebrarum, tensor tarsi, and corrugator supercilii.
Four pairs belong to the nose; viz. pyramidalis nasi, levator labii superioris alseque nasi, compressor and depressor naris.
Three pairs belong to the upper lip; viz. levator labii superioris, levator anguli oris, and depressor labii superioris.
Three pairs belong to the lower lip; viz. depressor anguli oris, depressor labii inferioris, and levator labii inferioris.
Three pairs to the mouth; viz. zygomaticus major, minor, and buccinator; also one azygos, the orbicularis oris.
The deep muscles of the face which are connected with the lower maxilla and ares concerned in mastication, are the masseter, temporal, internal, and external pterygoid of each side.
We shall now proceed, in as brief terms as possible, to describe the attachments and functions of the most important of these muscles.
Occipito-frontalis. This is a single muscle, consisting of two symmetrical parts, coming from the back of the head and inserted into the front of it. It is placed immediately under the scalp, and has four bellies of muscular fibres, connected by a thick tendon. It arises from the superior semicircular ridges of the occipital bone, and is inserted into the superior margin of the orbicularis oculi, and of the corrugator supercilii; also into the os frontis and the roof of the nasal bones. Its object is to pull the skin backwards and forwards, throwing that of the forehead into horizontal wrinkles; it elevates the eyebrows.
The common muscles of the ear are: 1. Superior auris, or attollens aurem, arising from the cranial aponeurosis, and inserted into the upper and antrior part of the cartilage of the ear; its use is to raise the cartilage, and to stretch the epicranial fascia. 2. Anterior auris, or attrihens aurem; this arises from the posterior part of the zygomatic process, and from the cranial aponeurosis, and is inserted into the anterior part of the helix. Use: to draw the external ear forwards and upwards. 3. Posterior auris, or retrahens aurem, arises from the mastoid process above the sternomastoid muscle, and is inserted into the back part of the concha. Use: to enlarge the meatus of the ear, and to direct it backwards.
Orhicidaris, or sphincter palpehrarum. This is a broad circular muscle, lying immediately under the skin of the eyelids. The first point of this muscle is principally the ligamentum palpebrale internum, and the internal canthus of the orbit; elsewhere it is but loosely attached to the subjacent parts.
Tensor tarsi. This arises from the posterior edge of the os unguis, passes forwards, and is inserted into the lachrymal ducts. Use: to draw the puncta and eyelids in close contact with the eye, and to press the former upwards the nose; this muscle is sometimes called Horner’s muscle, from its discoverer.
Corrugator supercilii arises from the internal angular process of the os frontis, and is inserted into the middle of the eyebrow, mixing with the orbicularis and occipito-frontalis muscles. Use: to depress and approxipiate the eyebrows, throwing the skin into vertical wrinkles, as in frowning.
Pyramidalis nasi arises from the occipito-frontalis, and is inserted into the compressor nasi muscle. Use: to raise the skin covering the ossa nasi.
Compressor nasi is a thin and triangular muscle, placed on the side of the nose, between the skin and the cartilage; it arises from the inner side of the canine fossa, in the superior maxilla, and is inserted by a thin aponeurosis into the dorsum of the nose, joining some fibres from the opposite side; its use is to press the ala towards the septum, or to draw it from it, so as alternately to enlarge or diminish the anterior nares.
Levator labii superioris alceque nasi is a long, thin, triangular muscle, placed on the side of the nose, between the orbit and the upper lip; it arises from two ridges: first, from the upper extremity of the nasal process of the superior maxilla; second, from the edge of the orbit above the infra-orbital hole; it is inserted into the ala nasi, and into the upper lip and orbicularis oris; its use is indicated by the name.
Zygomaticus minor is very small, and sometimes wanting; it arises from the upper part of the malar bone, and is inserted into the upper lip, near the commissure. Use: to draw the angle of the mouth upwards and outwards, as in smiling.
Levator anguli oris (musculus caninus) is situated about the middle of the face; it arises from the canine fossa in the superior maxillary bone, immediately below the infra-orbital foramen, and above the alveolus of the first molar tooth, and is inserted into the commissure of the lips, and into the orbicularis oris.
Depressor labii superioris alæque nasi. This arises from the myrtiform fossa in front of the alveoli of the canine and incisor teeth of the upper maxilla, and is inserted into the integuments of the upper lip, and into the fibro-cartilage of the septum and ala nasi. Use: to press the lips against the anterior teeth, and to depress the septum and ala nasi.
Depressor anguli vel triangularis oris is a flat and triangular muscle, situated at the lower part of the face; it arises from the external oblique line on the outer side of the lower jaw, which extends from the anterior edge of the masseter muscle to the mental foramen; its insertion is into the commissure of the lips; its name denotes its use.
Depressor labii inferioris vel quadratics menti is broad and somewhat square; arises from the side and front of the lower maxilla, and is ifiserted into half the lower lip, and into the orbicularis oris; it conceals the following muscle.
Levator labii inferioris vel menti arises from the alveoli of the lower incisors, by the side of the symphysis; it is inserted into the integument of the chin; its use is to elevate the chin and lower lip.
Orbicularis vel sphincter oris surrounds the opening of the mouth, and consists of two fleshy fasciculi, one for each lip, whose fibres decussate at the commissures, and intermix with all the dilating muscles inserted there; its use is to approximate the lips, and regulate their motion in the acts of speaking and breathing. This muscle has no bony attachment.
Buccinator. This is broad, thin, and somewhat square; situated between the two alveolar arches, it forms the inner side of the cheek and the lateral boundary of the mouth, lying close to the mucous membrane of the latter. It arises from the two posterior alveoli of the superior maxilla, from the external surface of the posterior alveoli of the lower maxilla, and from a strong aponeurosis (the pterygo-, or inter-maxillary ligament). It is inserted into the commissure of the lips; its uses are to press the cheek against the teeth, and to assist in other operations of mastication and articulation.
The first of the deep-seated muscles of the face is the masseter. This strong muscle covers the ramus and angle of the jaw, and consists of two parts, one anterior, the other posterior. The anterior arises from the superior maxilla where it joins the malar bone, and from the inferior edge of the latter, and is inserted into the outer surface of the angle of the lower maxilla. The posterior portion arises from the edge of the malar bone, and is inserted into the external side of the angle and ramus of the jaw. When both portions of both muscles act together, they elevate the lower jaw; if the anterior portions only of opposite sides act, they carry the face forwards and upwards; if the posterior alone act, they carry it backwards and upwards; if the superficial layer of one side act alone, it can rotate the chin to the opposite side; and if the deep layer only act, it can rotate the chin to its own side.
The temporalis is concealed by the temporal aponeurosis, the zygoma, and the masseter; it fills the temporal fossa, and arises from all sides of the cranium beneath the semicircular ridge on the parietal bone, and from all the temporal fossa and fascia; it is inserted by a strong tendon into the coronoid process of the inferior maxilla; it nearly surrounds that process, except on its outer side, and is continued along its fore part as far as the last molar tooth; its principal use is to raise the lower jaw, but it may assist to move the jaw forwards, backwards, and laterally.
Pterygoideus internus is situated on the inner side of the ramus of the jaw: it arises from the inner side of the external pterygoid plate and pterygoid process of the palate Done; it fills the greater part of the pterygoid fossa, and is inserted into the inner side of the angle of the jaw. Its use is to draw forward and elevate the jaw, and to rotate it.
Pterygoideus externus arises from the outer side of the external pterygoid plate, from the crest on the root of the great wing of the sphenoid, and from the back part of the tuberosity of the superior maxilla; it is inserted into the anterior and internal part of the neck of the lower jaw, into the inter-articular cartilage, and into the inferior synovial membrane. Its use is to draw forward the jaw with the inter-articular cartilages: when both muscles act alternately, they become the principal agents in grinding the food.
Pl. 127, fig. 1, superficial muscles of the head from the left side: 1, epicranial aponeurosis; 2, 3, occipito-frontalis, anterior portion; 4, posterior portion, the two connected by the epicranial aponeurosis; 5, attollens aurem; 6, retrahens aurem; 7, attrahens aurem; 8, orbicularis palpebrarum; 9, compressor naris; 10, levator labii superioris alseque nasi; 11, levator labii superioris; 12, zygomaticus minor; 13, zygomaticus major; 14, levator anguli oris; 15, depressor anguli oris; 16, depressor labii inferioris; 17, levator menti; 18, orbicularis oris; 19, buccinator; 20, masseter.
Fig. 2, deep-seated muscles of the head from the left side: 1, temporal muscle; 2, corrugator supercilii; 3, superior oblique muscle of the eye; 4, levator palpebrse; 5, compressor naris; 6, depressor naris; 7, orbicularis; 8, levator anguli oris; 9, depressor labii inferioris; 10, buccinator.
Pl. 124, fig. 15 1, epicranial aponeurosis; 2, occipito-frontalis; 3, compressor naris; 4, levator labii superioris alseque nasi; 5, levator proprius labii superioris; 6, orbicularis; 7, depressor anguli oris; 8, depressor labii superioris; 9, transversus menti (of rare occurrence); 10, attollens aurem; 11, attrahens aurem; 12, orbicularis palpebrarum; 13, zygomaticus major; 14, zygomaticus minor.
Fig. 16 1, occipital portion of occipito-frontalis; 2, retrahens aurem.
Fig. 171, occipital portion of occipito-frontalis.
Pl. 125, fig. 19 1, temporalis; 2, levator palpebræ superioris; 3, zygomaticus; 4, orbicularis; 5, levator anguli oris; 6, masseter.
Fig. 201, temporal muscle.
Pl. 126, fig. 20 1, orbicularis; 2, buccinator; 3, levator menti.
Muscles of the Neck
The neck is that contracted portion of the trunk between the head and chest, the cervical vertebræ forming its skeleton or support. Its anatomy is very intricate, containing numerous muscles, nerves, and vessels, besides the pharynx, œsophagus, larynx, and trachea. The muscles on the back of the neck will be considered with those of the back of the trunk. We shall confine ourselves to those of the anterior and sides.
The muscles of the anterior part of the neck are very numerous, and are concerned in the performance of various functions. Some act as muscles of locomotion, others are engaged in deglutition, in respiration, and in the exercise of voice and speech. They are symmetrical or similar on each side of the median line, and are twenty-one pairs in number, arranged in three layers, a superficial, middle, and deep. The superficial consists of two pairs, the platysma myoides and sterno-cleido-mastoid. The middle may be divided into two orders, the inferior and superior. The inferior are three: the sterno-hyoid, sterno-thyroid, and omo-hyoid; the superior are nine: digastric, mylo-hyoid, genio-hyoid, three styloid muscles, and the hyo-glossus, genio-hyo-glossus, and lingualis muscles. The deep layer consists of seven pairs: longus colli, rectus capitis, anticus major and minor, rectus lateralis, and three scaleni. This arrangement excludes the muscles of the palate, pharynx, and larynx.
The platysma myoides, or latissimus colli, is a thin, pale, cutaneous muscle, weak and indistinct in many subjects; it is situated on the fore part and side of the neck, extending from the chest and shoulder to the face; it arises by many fine fibres from the cellular membrane covering the upper part of the deltoid and pectoral muscles. It is inserted, first, into the skin and cellular tissue of the chin; second, into the fascia along the sides of the lower jaw; third, into the fascia which covers the parotid, and which adheres to the meatus auditorius. Its use is to depress the angle of the lip and the lower jaw, as also to compress and support the several muscles, glands, and vessels in the region of the neck.
The sterno-cleido-mastoideus is situated at the anterior and lateral part of the neck: it arises by a strong flat tendon from the upper and anterior part of the first bone of the sternum, also from the upper edge of the clavicle, and is inserted into the upper part of the mastoid process, and into the superior transverse ridge of the occipital bone. The sternal portion can rotate the head so as to turn the face towards the opposite side; the clavicular can bend the head and neck, so as to approximate the ear and shoulder. Both portions acting together on each side will move the head downwards and forwards.
The sterno-hyoideus, a long, flat, and thin muscle, arises within the thorax from the posterior surface of the first bone of the sternum and sternal end of the clavicle, and is inserted into the lower border of the body of the os hyoides, internal to the omo-hyoid. Use: to depress the os hyoides, pharynx, and larynx.
The sterno-thyroideus is broader and shorter than the last: it arises from the posterior surface of the sternum and cartilage of the second rib, and is inserted into the oblique line on the ala of the thyroid cartilage. Its use is to depress the larynx.
The omo-hyoideus is a long and slender muscle, situated obliquely along the inferior, lateral, and fore part of the neck. It arises from the superior costa of the scapula behind its semi-lunar notch, and sometimes from the acromial end of the clavicle, and is inserted into the lower border of the os hyoides. Its use, in conjunction with its fellow on the opposite side, is to draw the os hyoides, pharynx, and larynx, downwards and backwards.
The digastricus, placed at the lateral and anterior part of the neck, thick and fleshy at each extremity, round and tendinous in the centre, arises from a groove in the temporal bone internal to the mastoid process, and is inserted into a rough depression on the inner side of the base of the jaw close to the symphysis. Its median tendinous portion passes through the stylohyoid muscle, and is connected with the corner of the hyoid bone by a dense fascia, and sometimes by a tendinous ring like a pulley. Its use is to depress the lower jaw, and when the mouth is closed to elevate the os hyoides, tongue, and larynx.
The mylo-hyoideus is a triangular muscle, arising from the myloid ridge on the inner surface of the sides of the maxilla, which line descends obliquely from the last "molar tooth towards the chin: it is inserted into the base of the os hyoides. Use: to elevate the os hyoides and tongue, so as to press the latter against the palate.
The genio-hyoideus, short and round, arises by a small tendon on the inner side of the chin, above the digastric, and descending, is inserted into the base of the os hyoides. Its use is to draw the os hyoides upwards and forwards, to push the tongue against the incisor teeth, or to protrude it from the mouth.
The hyo-glossus is flat and thin, arising from the corner and part of the body of the os hyoides, and being inserted into the side of the tongue. Use: to render the dorsum of the tongue convex by depressing its side; it may also elevate the os hyoides and base of the tongue.
The genio-hyo-glossus is triangular or fan-shaped: it arises by a small tendon from an eminence inside the chin beneath the frasnum linguæ: the insertion is into the mesial line of the tongue from the apex to the base, and into the body or lesser corner of the os hyoides. This muscle is of importance in mastication and deglutition, as also in the articulation of certain letters.
Lingualis is a fasciculus of fibres taking a longitudinal course on the inferior surface of the tongue from the base to the apex; its use is to shorten the tongue and bend the tip downwards and to one side.
Stylo-hyoideus arises from the outer side of the styloid process near its base, and is inserted into the cornu and body of the os hyoides. It cooperates with the digastric in raising and drawing back the os hyoides and tongue.
Stylo-glossus arises from the inner side of the styloid process near its point, and is inserted into the side of the tongue. It draws the tongue backwards and to one side, and raises the tip behind the upper incisors.
Stylo-pharyngeus arises from the back part of the root of the styloid process, and is inserted into the side of the pharynx, also into the corner of the os hyoides and thyroid cartilage. It elevates and dilates the pharynx so as to receive the food from the tongue.
Longus colli, the first of the deep layer of the muscles of the neck, extends from the third dorsal vertebra to the atlas: it arises from the sides of the bodies of the three superior dorsal and four inferior cervical vertebræ, from the intervertebral ligaments, also from the head of the first rib and irom the anterior tubercles of the transverse processes of the last four cervical vertebræ. The fibres ascend obliquely, adhering to each bone in their course, and are inserted into the fore part of the first, second, and third cervical vertebræ. Use: to bend the neck on one side, and rotate the athis on the vertebra dentata; when both muscles act, they bend the neck directly forwards.
Rectus capitis anticus major, long and flat, thick above and below, arises by small tendons from the anterior tubercles of the transverse processes of the last four cervical vertebræ; they soon unite in a fleshy substance, which is inserted into the cuneiform process of the occipital bone. It serves to bend forwards the head and neck.
Rectus capitis anticus minor, short and narrow, arises from the transverse process of the atlas, and is inserted into the cuneiform process. It serves to bend the head forwards and to one side on the atlas.
Rectus capitis lateralis, very short, arises from the transverse process of the atlas, and is inserted into the semilunar ridge or jugular process of the occipital bone which extends from the condyle to the mastoid process. With the last muscle it serves to bend the head forwards or to incline it to one side.
Scalenus anticus, in part continuous with the rectus anticus major, arises from the anterior tubercles of the transverse processes of the third, fourth, fifth, and sixth cervical vertebræ; the fibres descending form a flat muscle, which is inserted tendinous into the upper surface of the first rib, near its cartilage. Its use is to bend the neck forwards and laterally, also to elevate and fix the rib, as in inspiration.
Scalenus medius, larger and longer than the last, arises from the posterior tubercles of the transverse processes of four or five inferior cervical vertebræ, and is inserted into the upper surface of the first rib, behind the subclavian artery. Its use is similar to that of the last.
Scalenus posticus arises from the posterior tubercles of two or three lower cervical vertebræ, and is inserted into the upper edge of the second rib, between the tubercle and angle. Use: to elevate the second rib; to bend the neck to one side and a little backwards.
Pl. 127, fig. 3 1, platysma myoides; 2, branch of the latter known as musculus risorius santorini; 3, sterno-cleido-mastoid; 4, trapezius.
Fig. 41, 2, the digastric muscle.
Pl. 124, fig. 1516, platysma myoides.
Pl. 125, fig. 197, sterno-cleido-mastoid.
Muscles of the Anterior and Lateral Parts of the Thorax
The thorax is the middle division of the body, continuous with the neck above and the abdomen below; it presents an anterior or sternal, a posterior or dorsal, and two lateral aspects.
Pectoralis major, flat and triangular, arises from the sternal half of the clavicle, from the anterior surface of the sternum, from the cartilages of the third, fourth, fifth, and sixth true ribs, and from an aponeurosis common to it and to the external oblique muscle; its fibres are inserted by a flat tendon into the anterior edge of the bicipital groove, and by an aponeurosis into the fascia of the arm. A line of cellular membrane separates the clavicular from the sternal portion, these in some cases appearing as distinct muscles. It serves important purposes in moving the arm and in inspiration.
Pectoralis minor, flat and triangular, arises from the external surface and upper edge of the third, fourth, and fifth ribs, external to their cartilages, and is inserted into the inner and upper surface of the coracoid process of the scapula, near its anterior extremity, being here connected with the coraco-brachialis and short head of the biceps. Use: to draw the shoulder forwards, downwards, and upwards, also to assist the pectoralis major in elevating the ribs in inspiration.
Subclavius, small and round, arises by a flat tendon from the cartilage of the first rib, external to the rhomboid or costo-clavicular ligament; it is inserted into the external half of the inferior surface of the clavicle. Its use is to draw the clavicle and shoulder forwards and downwards; also to elevate the first rib in inspiration, if the shoulder and clavicle be raised and fixed.
Serratus magnus, thin and broad, placed between the scapula and the ribs, arises by eight or nine fleshy strips from the eight or nine superior ribs; the fibres ascending are inserted between the subscapular, rhomboid, and levator anguli muscles into the base of the scapula, but particularly into the superior and inferior angles. It depresses the scapula and draws it forwards, raising the acromion process and the shoulder joint by rotating the scapula on its axis; it also plays an important part in inspiration.
Intcrcostales are twenty-two in number on each side, eleven external and eleven internal. The external commence at the transverse processes of the dorsal vertebræ, arise from the inferior edge of each rib, and are inserted into the external lip of the superior edge of the rib beneath. The internal intercostals take an opposite direction and decussate the former; they commence at the sternum and are discontinued at the angles of the ribs. They arise from the inner lip of the lower edge of each cartilage and rib, and are inserted into the inner lip of the superior edge of the cartilage and rib beneath. Both laminæ co-operate to raise the ribs, the first rib being fixed by the scaleni.
Levatores costarum arise from the extremity of each dorsal transverse process, and are inserted into the upper edge of the rib beneath, between its tubercle and angle. They serve to elevate the ribs.
Triangularis sterni, or sterno-costalis, arises from the posterior surface and edge of the lower part of the sternum, and from the xiphoid cartilage, and is inserted into the cartilages of the fourth, fifth, and sixth ribs. Use: to depress and draw back the cartilages of the ribs, so as to assist in expiration.
Pl. 127, fig. 9 1, pectoralis major; 2, pectoralis minor; 3, subclavius; 4, serratus magnus; 5, intercostals.
Pl. 124, fig. 1518, pectoralis major. Fig. 177, serratus magnus.
Pl. 125, fig. 19 8, subclavius; 9, pectoralis minor; 10, dentations of the serratus magnus.
Pl. 126, fig. 2015, 16, intercostals.
Muscles of the Back
The muscles of the back are many of them indistinct, and vary considerably in different bodies. They are symmetrical on each side, and may be arranged in four successive layers, each nearly covering the other, between the integuments and the bones. The muscles of the first layer are two in number.
The trapezius, broad and triangular, with the base along the spine, the apex at the shoulder, arises from the internal third of the superior transverse ridge of the occipital bone, from the ligamentiim nuchas, and from the spinous processes of the last cervical and of all the dorsal vertebræ; it is inserted into the posterior border of the external third of the clavicle and of the acromion process of the scapula. Its use is to raise and draw backwards the shoulder.
The latissimus dorsi is triangular and very broad, covering the greater part of the lumbar and dorsal region; it arises from all the lumbar spines and supra-spinal ligaments, also from the pelvis and last three or four ribs; its insertion is into the concave surface and into the inner or posterior edge of the bicipital groove. Use: to depress the shoulder and arm, to draw the arm backwards and inwards, to rotate the humerus inwards, &c.
The second layer of muscles consists of the rhomboid, levator anguli scapulæ, serratus inferior and superior, and the splenii.
Rhomboideus is broad and thin, and is the most superficial of this layer; it is divided into a superior or minor portion, and an inferior or major; the former arises from the lower part of the ligamentum nuchae, and from the two last cervical spinous processes, and is inserted into the base of the scapula, opposite to and above the spine; the major portion arises from the four or five superior dorsal spines, and is inserted into a thin tendinous arch, extending along the base of the scapula from its spine to its inferior angle. Use: to draw the shoulder backwards and upwards.
Levator anguli scapulcæ is a long and flat muscle, placed at the upper and posterior part of the side of the neck; it arises from the posterior tubercles of the transverse processes of the four or five superior cervical vertebræ, and is inserted into the base of the scapula, between the spine and the superior angle; its use is to elevate the whole scapula, when it is assisted by the trapezius, or alone, to raise the superior angle.
Serratus posticus superior is placed on the superior posterior part of the thorax, arises from the ligamentum nuch and from two or three dorsal spines, and forms a thin fleshy belly ending in three fleshy strips, which are inserted into the upper borders of the second, third, and fourth ribs, external to their angles. Use: to expand the thorax by elevating the ribs, and drawing them outwards.
Serratus posticus inferior, at the lower part of the dorsal and upper part of the lumbar regions, arises by a tendinous expansion, connected through the lumbar fascia to the two last dorsal and two upper lumbar spines. Its three or four fasciculi are inserted into the lower edges of the four inferior ribs, anterior to their angles; its use is to assist the abdominal muscles in expiration, and the diaphragm in inspiration.
Splenius is long, fleshy, and tendinous, lying beneath the trapezius; it is divided about its centre into two portions: the inferior or splenius colli, and the superior or splenius capitis. The former arises from the spines of the third, fourth, fifth, and sixth dorsal, and is inserted into the transverse processes of the three or four superior cervical vertebræ. The latter arises from the spinous processes of the two superior and dorsal, and three inferior cervical vertebræ, and is inserted into the back part of the mastoid process. The use of the splenius muscles is to bend back the head; and where one only acts, to turn the head to that side.
The next layer of muscles consists of the sacro-lumbalis, longissimus dorsi, spinalis dorsi, cervicalis descendens, transversalis colli, trachelo-mastoideus, and complexus.
Sacro-lumbalis, longissimus dorsi, and spinalis dorsi are so closely connected inferiorly as to appear but one mass; they fill the hollow between the angles of the ribs and the spinous processes; the first is external, the second in the middle, and the third internal. They serve to strengthen the spine, and to assist in respiration.
Cervicalis descendens or ascendens arises internal to the sacro-lumbalis, by four or five tendons, from as many of the superior ribs, between their tubercles and angles; it is inserted into the posterior tubercles of the transverse processes of the fourth, fifth, and sixth cervical vertebræ. Use: to extend the neck, and incline or turn it to one side; it may also assist in respiration.
Transversalis colli arises internal to the longissimus dorsi, by small slips, from the transverse processes of five or six superior dorsal vertebræ; it is inserted by small tendons into the transverse processes of four or five inferior cervical vertebræ; its use is nearly similar to that of the last described muscle.
Trachelo-mastoideus, like a continuation of the longissimus dorsi, lies internal to the last, and external to the next. It arises from the transverse processes of three or four superior dorsal vertebræ, and from as many inferior cervical; ascending, it is inserted into the inner and back part of the mastoid process, beneath the insertion of the splenius; it assists in extending the neck, in bringing the head backwards, and inclining and rotating it to one side.
Complexus is thick and strong, and arises from the transverse and oblique processes of three or four inferior cervical, and five or six superior dorsal vertebra, internal to the transversalis and trachelo-mastoideus; it is inserted close to its fellow into the occipital bone, between the two transverse ridges. Use: to draw back the head; to fix and support it on the spine; also, to rotate it as antagonistic to the splenius.
Spinalis, or semi-spinalis colli, is one of the largest muscles in this region. It arises from the extremity of the transverse processes of five or six superior dorsal vertebræ, and is inserted into the spmous processes of the second, third, fourth, and fifth cervical vertebræ; its use is to extend the neck, and incline it to its own side.
Semi-spinalis dorsi is similar to the last mentioned muscle in form, attachment, and function.
Multifidus spinæ is close to the vertebra), between the spinous and the transverse processes. It consists of a series of small tendinous and fleshy fasciculi; the first arises from the spine of the dentatus, and is inserted into the transverse process of the third; the last arises from the spine of the last lumber vertebra, and is inserted into the false transverse process of the sacrum. It supports the spinal column, strengthens it, and inclines it to one side.
Interspinales are short muscles, consisting of longitudinal fibres, whose attachment is indicated by the name; they support and extend the spine.
Intertransversales consist of longitudinal fibres, attached and situated as implied by the name. Use: to support the spine on either side, and to bend it laterally.
Rectus capitis posticus major is a triangular muscle, arising from the spinous process of the second vertebra; it is inserted into the inferior transverse ridge of the occipital bone. Use: to extend the head or draw it backwards, also to rotate it and the atlas on the second cervical vertebra.
Rectus capitis posticus minor, also triangular, arises from the posterior part of the atlas, and is inserted into the occipital bone, behind the foramen magnum. Use: to assist the preceding muscle in drawing back the head and steadying it on the spine.
Ohliquus capitis inferior is the strongest of these small muscles; it arises inferiorly and externally to the posterior rectus, from the spinous process of the second vertebra, and is inserted into the extremity of the transverse of the atlas. Use: to rotate the head and atlas on the second vertebra.
Obliquus capitis superior arises from the upper part of the transverse process of the atlas, and is inserted into the occipital bone, between its transverse ridges, and just behind the mastoid processes. Use: to bend the head to one side, and to draw it a little forwards.
Pl. 124, fig. 16 4, trapezius; 16, latissimus dorsi.
Pl. 125, fig. 20 2, splenius; 3, levator scapulæ; 4, rhomboideus; 5, serratus posticus superior; 9, serratus posticus inferior; 10, quadratus lumborum.
Pl. 126, fig. 21 1, rectus capitis posticus minor; 2, rectus capitis posticus major; 3, obliquus capitis superior; 4, obliquus capitis inferior; 5, biventer cervicis and complexis; 6, seraispinalis colli; 7, scalenus posticus; 8, trachelo-mastoid; 9, transversalis colli: 10, cervicalis descendens or ascendens; 18, multifidus spinæ; 19, semispinalis dorsi; 20, spinalis dorsi; 21, 22, levatores costarum; 23, intertransversalis; 24, posterior attachment of the transversalis abdominis; 25, 2019, pl. 127, fig. 1112, quadratus lumborum.
Pl. 128, fig. 1 1, serratus posticus superior; 2, serratus posticus inferior; 3, dorsal aponeurosis; 4, splenius capitis; 5, 6, sacro-spinalis; 7, cervicalis ascendens; 8, trachelo-mastoid; 9, semi-spinalis dorsi et colli; 10, complexus; 11, spinalis dorsi et colli.
Fig. 2 1, splenius capitis; 2, splenius colli; 3, 5, complexus; 4, trachelo mastoid.
Fig. 3 1, complexus; 2, traclielo-mastoid; 3, minor, 4, major rectus capitis posticus; 5, obliquus capitis, inferior and superior.
Muscles of the Abdomen and Pelvis
The abdominal and pelvic muscles proper may be divided into the superficial, consisting of the obliquus externus and internus, transversalis, rectus, and pyramidalis of each side, and the deep-seated viz. the quadratus lumborum, psoas parvus and magnus, and iliacus internus of each side, and the diaphragm.
The obliquus externus, or descendens, broad, thin, and somewhat square, extends over the anterior and lateral part of the abdomen. It arises by eight or nine triangular fleshy slips from the lower edges and external surface of the eight or nine inferior ribs at a little distance from their cartilages; this serrated origin is in the form of a long curved line, the concavity upwards and backwards. The insertion is into the xiphoid cartilage, linea alba, pubes, Poupart’s ligament (formed by a thickening and reflection or folding back of the lower fibres of this tendon), and into the anterior superior spinous process of the ilium, also into the outer edge of the two anterior thirds of the crest of the ilium. Use: to depress and abduct the ribs, and to compress the abdominal viscera so as to assist in expiration and in the evacuation of the urine and fasces. The linea alba is a dense ligamentous cord extending from the ensiform cartilage to the upper part of the symphysis pubis, and is formed by the intimate union and crossing of the tendinous fibres of the two oblique and transverse muscles of opposite sides. The lineæ semi-lunares extend from the tuberosity of the pubes on each side, about four inches from the linea alba, towards the cartilages of the eighth and ninth ribs. They appear white and somewhat depressed, and are formed by the tendons of the internal oblique, dividing at the edge of each rectus into two layers, to inclose the muscle in a sort of sheath. The lineæ transversæ are three or four on each side; they cross the rectus muscle from the linea alba to the line semi-lunares; they are tendinous intersections of that muscle, particularly of its anterior part, which adhere so intimately to its sheath as to give the latter this indented appearance. Poupart’s ligament, as already remarked, is the inferior edge of the tendon of the external oblique, thickened and reflected. Considered as a distinct ligament, it may be said to arise from the anterior superior spinous process of the ilium, and passing forwards and inwards, to be inserted into the pubes by two attachments; one anteriorly into the tuberosity or spine, the other principally into the innominata of the pubes. This second insertion is sometimes known as Gimbernaut’s ligament.
Obliquus internus or ascendens is also situated at the anterior and lateral part of the abdomen, broader before than behind. It arises from the fascia lumborum, from all the crest of the ilium, and from the two external thirds of the grooved or abdominal surface of Poupart’s ligament, and is inserted into the cartilages of the four inferior ribs, the xiphoid cartilage, the cartilage of the seventh and eighth ribs, and the whole length of the linea alba: its tendon conjoined with that of the transversalis is inserted into the symphysis and upper edge of the pubcs, as also into the linea innominata. The use of this muscle is to assist the external oblique in expiration by depressing the ribs; also to bend the trunk forwards or to one side.
The cremaster or suspensorius testis, hardly a distinct muscle, and only rudi mental in the female, consists of a fasciculus of pale fleshy fibres which arise from the internal surface of the external third of Poupart’s ligament, and from the lower edge of the obliquus internus; the fibres pass downwards and forwards around the spermatic cord, and are inserted into the tunica vaginalis; a few fibres are lost in the scrotum. Use: to support, compress, and raise the testicle and its vessels.
Transversalis, a somevhat square muscle, arises from the fascia lumborum and the posterior part of the crest of the ilium, and from the iliac third of Poupart’s ligament; also from the two last ribs, and by fleshy slips from the inner side of the succeeding five. All the fibres end in a flat tendon, which near the lineæ semi-lunares joins the posterior lamina of the internal oblique, and is inserted along with it into the whole length of the linea alba, into the upper edge of the pubes, and also into the linea innominata. Its use is to compress the abdominal viscera in the circular direction, and to assist in expiration.
The rectics abdominis is a long and flat muscle situated in the anterior part of the abdomen. It arises by a flat tendon, which is sometimes double, from the upper and anterior part of the pubes, between the spine and symphysis; it ascends parallel with its fellow, and is inserted into the anterior part of the thorax by three fasciculi. Of these, the internal is fixed to the cartilage of the seventh rib and costo-xiphoid ligament; the middle to the cartilage of the sixth rib; and the external to the cartilage of the fifth rib. It use is to bend the chest towards the pelvis, and to compress the abdomen.
The pyramidalis, sometimes wanting, arises from the symphysis pubis, and from the upper edge of the bone external to it, and is inserted into the linea alba, midway between the umbilicus and pubes. Use: to assist the rectus and make tense the linea alba.
The diaphragm, the first of the deep muscles of the abdomen, is one of the most important in the body, second only to the heart. It is the principal agent in respiration, and is in a measure only under the influence of volition. It is usually divided into two portions, one superior, large, and broad transversely (the true or costal diaphragm); the other is inferior and posterior, small, thick, and narrow (the appendix, crura, or vertebral diaphragm). These two portions, although separate at their osseous attachments, are yet blended together in the common central tendon and present a fan-shaped expansion, bent at their junction, the broad superior portion being nearly horizontal, while the posterior inferior is vertical and joined to the former at nearly a right angle. The superior arises. The central or cordiform tendon of the diaphragm is of considerable extent, and is entirely surrounded by fleshy fibres. Below this tendon are the two crura or appendices, nearly parallel to the spine. There are three large openings in the diaphragm: one for the aorta (hiatus aorticus), of a semi-lunar form, and in the median line; one for the inferior vena cava (foramen vence cavæ or quadrilaterum), nearly square, and to the right side; and one for the œsophagus (hiatus œsophageus), elliptical, and to the left side.
The quadratics lumborum is a thick, flat, irregularly, square muscle, situated in the lumbar region next the spine, forming part of the posterior wall, of the abdomen. It arises from the posterior fourth of the crest of the ilium and from the ilio-lumbar ligament; it is inserted into the extremity of the transverse processes of the four first lumbar vertebræ and of the last dorsal. Its use is to bend the spine to one side, to depress the last rib, and thus assist in expiration; both muscles acting together support the spine.
Psoas parvus, a long, thin, and narrow muscle, is situated behind the psoas magnus and arises from the lower edge of the side of the body of the last dorsal vertebra, also from the body of the first lumbar, and the inter-vertebral substance; it ends in a thin tendon which crosses the psoas magnus and is inserted into the ilio-pectineal eminence and adjacent part of the brim of the pelvis. Use: to assist in bending forwards the body or in raising the pelvis.
Psoas magnus extends along the sides of the lumbar vertebræ, the brim of the pelvis, and the anterior and inner part of the thigh, as a long, round, and fleshy muscle. It arises by two planes of fasciculi, the one anterior from the sides of the border of the two last dorsal and four first lumbar vertebræ; the other posterior, from the bases of the transverse processes. The fibres become attached to a tendon in common with those of the iliacus muscle, which passing around the hip joint becomes inserted into and around the lesser trochanter of the femur. Its use is to flex the thigh on the pelvis, or the pelvis on the thigh; in standing it supports the spine and prevents its bending backwards; it is especially concerned in walking.
The iliacus internus, a flat, radiated, or triangular muscle, arises from the transverse process of the last lumbar vertebra, ilio-lumbar ligament, base of the sacrum, inner margin of the crest of the ilium, the brim of the acetabulum, &c., and is inserted into the common tendon of the psoas magnus as already described. It assists the psoas in flexing and rotating the thigh.
We next proceed to the consideration of the perinæal muscles, the first of which is the sphincter ani externus, a flat, thin, oval muscle, open in the middle. It arises from a fibro-cellular substance extending from the os coccygis to the rectum (recto-coccygeal ligament), and encircling the anal orifice, is inserted into the raphe or prominent hard ridge of the perinaeum and into the superficial fascia. It serves to close and raise the anus, also to draw the bulb of the urethra downwards and backwards, and to compress it.
The sphincter ani internus vel orbicularis is a thick fasciculus of muscular fibres, encircling the lower extremity of the rectum, with no attachment to the rectum behind, and only a slight one to the central point before, but is in close contact with the mucous membrane of the intestine. Its use is to assist the former muscle in closing the extremity of the rectum in defecation.
Erector or compressor penis, a long and flat muscle, arises from the inner surface of the tuber ischii, and from the insertion of the great or inferior sacro-sciatic ligament: it is inserted into the fibrous membrane of the corpus cavernosum of the penis. Its use is to draw down and facilitate the erection of the penis.
Accelerator urinæ, or ejaculator seminis, extends from the front of the rectum to the back part of the scrotum, and is attached to its fellow along the mesial line. Use: to expel the last drops of semen or urine.
Transversalis perinæi is a thin and weak muscle, sometimes wanting: it arises from the inside of the tuberosity of the ischium above the erector penis muscle, and is inserted into the central portion of the perinseum behind the accelerator urinæ. It supports and raises the anus, assisting also in defecation.
Levator ani is a flat, thin, and broad muscle, placed at the inferior and lateral part of the pelvis. It arises by three origins, the first from the posterior part of the symphysis pubis, the second from the obturator fascia and the ilium, the third from the inner surface of the ischium: it is inserted into the central point of the perinseum, and into the fore part of the rectum, into the sides of the rectum, and into the back part of the rectum, as also into the two last bones of the coccyx. Its use is to raise and draw forward the rectum, as also to close it; it also assists powerfully in the evacuation of fæces, urine, and semen.
The coccygeus is a small triangular muscle posterior to the levator ani: it arises from the inner surface of the spine of the ischium, and is inserted into the extremity of the sacrum and side of the coccyx. It supports and raises the coccyx in defecation, and assists in closing the inferior and posterior part of the pelvis.
Pl. 124, fig. 15 27, obliquus internus; 28, rectus abdominis. Fig. 178, obliquus externus.
Pl. 125, fig. 19 11, linea alba; 12, rectus abdominis crossed by the lineæ transversales; 13, trans versus abdominis.
Pl. 126, fig. 2018, transversus abdominis.
Pl. 127, fig. 9 6, obliquus externus; 7, femoral ring; 8, obliquus internus; 19, section of the aponeurosis of the obliquus externus; 11, linea alba. Fig. 10 1, 2, 3, obliquus internus; 4, 5, 6, transversus abdominis; 7, pyramidalis; 8, rectus abdominis; 9, linea alba. Fig. 11 1, muscular portion of the diaphragm; [2], central tendon or phrenic centre; 3, left crus; 4, right crus; 5, foramen venæ cavæ; 6, opening for the œsophagus; 7, do. for the aorta; 8, the posterior fibres of the true diaphragm, arising from 9, the ligamentum arcuatum; 10, psoas parvus; 11, psoas magnus; 12, quadratus lumborum; 13, iliacus internus.
Muscles of the Superior Extremities
The upper extremity is connected with the trunk by the sterno-clavicular ligaments, and by eleven muscles, all of which have been already described. Of these, one is connected to the clavicle (subclavius) two to the humerus (pectoralis major and latissimus dorsi), and eight to the scapula, viz. trapezius, levator anguli scapulæ, omo-hyoid, rhoraboides major and minor, serratus magnus, pectoralis minor, and latissimus dorsi. The muscles of the upper extremity are classed into those of the shoulder and arm, forearm, and hand.
1. Muscles of the Shoulder and Arm. These muscles are hidden from view by the supra-spinous, infraspinous, and subscapular fascise, and the brachial aponeurosis, which have already been briefly described. The proper muscles are six in number: the deltoid, supra and infra spinatus, teres minor and major, and the subscapularis. Those of the arm are four: the biceps, coraco-brachialis, brachialis anticus, and triceps.
The deltoides is a very thick, strong, and triangular muscle, bent so as to embrace the shoulder-joint in front, externally and behind. It arises from the lower edge of the spine of the scapula and from the anterior edge of the acromion process, and from the external third of the clavicle; its insertion is into a rough surface about two inches in extent situated on the outer side of the humerus, and commencing just above its centre. It abducts and raises the arm, draws it forwards or backwards, and rotates it inwards or outwards.
Supra-spinatus fills the fossa of the same name, and arises from all that portion of the scapula above its spine, as also from a strong fascia which covers the muscle; it is inserted into the upper and fore part of the great tuberosity of the humerus, into the most anterior and superior of the three depressions which are marked on that surface. It assists the deltoid in raising and abducting the arm, streng-thens the capsular ligament, and acts as antagonist to the pectoral, deltoid, and other muscles in preventing a tendency to dislocation.
Infra-spinatus is inferior to the last, flat, and triangular. It arises from the inferior surface of the spine of the scapula and from the dorsum of this bone as far down as the posterior ridge on the inferior costa; it is inserted into the middle of the external or greater tuberosity of the humerus below the infra-spinatus. Its use is to assist the superior part of the deltoid in raising tho, arm, drawing it backwards, and rotating it outwards; it also serves to strengthen the articulation.
Teres minor is a small muscle inseparably attached along the lower edge of the last muscle. It arises from a depression between the two ridges on the inferior costa of the scapula, and is inserted below the infra-spinatus into the inferior depression on the great tuberosity of the humerus, and into the bone a little lower down. It co-operates with the last muscle.
Sub-scapularis is a broad, triangular muscle, situated on the inner side of the scapula opposite to the three last mentioned muscles. It arises from all the surface and circumference of the subscapular fossa, and is inserted into the interval or small tubercle of the humerus. As the strongest of the capsular muscles, it strengthens the inner side of the articulation and guards against dislocation.
Teres major, a long and flat muscle, arises from a rough flat surface on the inferior angle of the scapula below the infra-spinatus, and is inserted into the inner or posterior edge of the bicipital groove, below the tendon of the latissimus dorsi. It rotates the humerus inwards, adducts and draws it downwards and backwards; it also draws forwards the inferior angle of the scapula.
The coraco-brachialis arises from the point of the coracoid process and from the tendon of the short head of the biceps; descending obliquely forwards, it is inserted into the inner side of the humerus, a little below the middle, and into the ridge leading to the internal condyle by an aponeurosis. It serves to adduct, raise, and draw forward the arm; also to rotate it outwards.
Biceps is situated along the fore part of the humerus, and consists of two portions superiorly, the external or long, and the internal or short. The internal arises from the coracoid process between the coraco-brachialis and the triangular ligament; the external or long head arises by a long tendon from the upper part of the glenoid cavity of the scapula; the two uniting about the middle of the humerus in a large fleshy belly, which ends in a flat tendon to be inserted into the back part of the tubercle of the radius. A process from the anterior and outer border of this tendon, called the semi-lunar fascia, passes to the internal cond3de and to the aponeurosis of the forearm. Its use is to flex the forearm and stretch its fasciæ; also to abduct and raise the arm.
Brachialis anticus or externus arises from the centre of the humerus by two fleshy slips, one on either side of the insertion of the deltoid; it is inserted by a strong tendon into the coronoid process of the ulna and into a rough surface on this bone beneath that process. Use: to flex the forearm, also to strengthen the articulation when extended.
Triceps extensor cubiti covers the back of the humerus, and extends from the scapula to the olecranon; it consists superiorly of three portions, the middle or long, the second or external, and the third or internal or short head (brachialis internus or posticus). The long or middle head arises from the lower part of the neck of the scapula; the second arises immediately below the insertion of the teres minor from and behind a ridge on the outer side of the humerus, commencing below the great tuberosity and leading down to the external condyle; the third or short head arises on the inside of the humerus above its centre. These three portions unite above the middle of the arm, and descending, terminate in a broad tendon of two laminæ, a superficial and a deep; the former is continued into the fasciæ on the back part of the forearm, the latter is inserted into the posterior border but not the point of the olecranon. Use: to extend the forearm on the arm, by its long portion to carry the arm backwards, and in some cases to abduct it. The triceps is thus the great extensor of the elbow joint, while the biceps and brachialis anticus are the antagonist flexors. The flexors thus predominate over the extensors, the contrary being the case in the knee joint.
2. Muscles of the Forearm. As these muscles are very numerous, they will be most conveniently described by classing them according to they situations and use. One set is employed in bending the forearm, wrist, and fingers: these are the flexors. A second, nearly allied to these, has the power of rolling the radius across the ulna, so as to turn the palm downwards: these are the pronators. The extensors can extend the forearm, hand, and fingers; and a fourth set, the supinators, can turn the palm of the hand upwards. The pronators and flexors arise chiefly from the internal condyle, and from the inner or ulnar side of the forearm.
The pronators and flexors arising from the inner side of the forearm are eight in number, arranged in a superficial and a deep layer. The superficial are the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum sublimis, and flexor carpi ulnaris. The deep are the flexor digitorum profundus, flexor pollicis longus, and the pronator quadratus.
Pronator radii teres arises from, the anterior part of the internal condyle and from the coronoid process of the ulna; it is inserted into the outer and back part of the radius about its centre. Use: to pronate the hand and bend the forearm.
Flexor carpi radialis arises from the inner condyle and from the intermuscular septa, and is inserted into the base of the metacarpal bone of the index finger.
Palmaris longus arises from the inner condyle, and is inserted into the annular ligament and the palmar aponeurosis. It bends the hand and stretches the palmar fascia.
Flexor carpi ulnaris arises from the internal condyle, and is inserted into the pisiform bone.
Flexor digitorum sublimis perforans arises from the internal condyle and internal lateral ligament, from the coronoid process, and from the portion of the radius below its tubercles and internal to the pronator teres. It ends in four tendons, two anterior for the middle and ring finger, and two posterior for the index and little finger; at the first phalanx of each finger, each tendon becomes inclosed in a strong sheath with one of the deep flexors. Near the end of the first phalanx, each superficial flexor tendon is split for the passage of the tendon of the deep flexor. Use: to flex the second joint of each finger on the hand, the hand on the forearm, and the forearm on the arm.
Flexor digitorum profundus perforans arises from the superior three fourths of the anterior surface of the ulna, and ends in four tendons, which pass beneath the annular ligament, and are inserted into the phalanges, as referred to when speaking of the last muscle. Use: to bend the last phalanx, and to co-operate with the superficial flexor in bending the other phalanges and the wrist.
Flexor pollicis longus arises from the fore part of the radius below its tubercle and from the interosseous membrane, to within two inches of the carpus. It is inserted into the middle of the last phalanx of the thumb, which it serves to flex.
Pronator quadratus is a small square muscle situated above the carpus, and arising from the inferior fifth of the internal and anterior surface of the ulna. It is inserted into the anterior part of the inferior fourth of the radius, and serves to roll the radius over the ulna.
The muscles situated on the outer and back part of the forearm are supinators and extensors, and may, like the last set, be arranged in a superficial and a deep layer. The superficial consists of seven: supinator radii longus, extensor carpi radialis longus and brevis, extensor digitorum communis, extensor minimi digiti, extensor carpi ulnaris, and anconæus. The deep muscles are five: the supinator radii brevis, three extensors of the thumb, and the indicator.
Supinator radii longus, forming the prominence along the other and anterior part of the forearm, arises from the external ridge of the humerus, and from the intermuscular ligament separating it from the outer head of the triceps. It is inserted into a rough surface on the outside of the radius, near its styloid process. It serves to roll the radius backwards and to bend the elbow joint.
Extensor carpi radialis longus arises from the ridge on the external side of the humerus, and is inserted into the back part of the metacarpal bone of the index finger.
Extensor carpi radialis brevis arises from the inferior and posterior part of the external condyle, and from the external lateral ligament; it is inserted into the carpal extremity of the third metacarpal bone (that of the middle finger).
Extensor digitorum communis arises with the last and the extensor minimi digiti, from the external condyle and from the ulna. About the middle of the back of the forearm it ends in four muscles, each ending in tendons, which pass under the annular ligament and are inserted into the phalanges of the four fingers. It serves to extend all the joints of the fingers, as also the carpus.
Extensor carpi ulnaris arises from the external condyle, fascia, and intermuscular septa, and ends in a strong tendon, which is inserted into the carpal end of the fifth metacarpal bone. It extends and bends back the hand, and adducts or flexes it laterally towards the ulna.
Anconæus is placed at the outer side of the olecranon, beneath the skin, and arises from the posterior and inferior part of the external condyle and lateral ligament, and is inserted into the external surface of the olecranon; and the superior fifth of the posterior surface of the ulna. Its use is to extend the forearm on the arm.
Extensor minimi digiti vel auricidaris arises in common with the extensor communis, and is inserted with the fourth tendon of this muscle into the posterior part of the phalanges of the little finger. It assists the extensor communis, and can extend and abduct the little finger independently of the rest.
Supinator radii brevis surrounds the upper part of the radius: it arises from the external condyle, external, lateral, and coronary ligaments, and from the outer side of the ulna, and is inserted into the external and anterior surface of the radius. It turns the radius outwards, so as to supinate the hand.
Extensor ossis metacarpi pollicis, or abductor pollieis longus, arises from the middle of the posterior part of the ulna and posterior surface of the radius, and is inserted by two tendons, one into the vtrapezium bone, the other into the upper and back part of the metacarpal bone of the thumb. It serves to extend the first joint of the thumb, and to separate it from the; fingers. It also assists in supination.
Extensor primi internodii pollicis, or extensor minor, arises from the back part of the ulna, below its middle, and from the interosseous ligament and the radius; it is inserted into the posterior part of the first phalanx. It serves to extend the second joint of the thumb, and to assist the last mentioned muscle.
Extensor secundi internodii pollicis, or extensor major, arises from the posterior surface of the ulna, above its centre, and from the interosseous membrane; it is inserted into the posterior part of the second or last phalanx; it extends, the last phalanx of the thumb upon the first.
Extensor indicts, or indicator, arises from the middle of the posterior surface of the ulna and interosseous membrane, and is inserted into the second and third phalanges of the fore finger. It assists the common extensor, or produces the extension of the fore finger alone, as in pointing.
3. Muscles of the Hand. These consist principally of the short muscles of the thumb and of the little finger, of the lumbricalis, and of the interosseous muscles.
The short muscles of the thumb are four in number, abductor pollicis, opponens pollicis, flexor pollicis brevis, and adductor pollicis, whose names, sufficiently indicate their use.
The muscles of the little finger are three, abductor minimi digiti, flexor brevis minimi digiti, and adductor or opponens minimi digiti.
The palmaris brevis is placed just below the skin, at the inner side of the palm of the hand; it consists of separate fasciculi which arise from the anterior ligament of the wrist, and is inserted into the skin and fat at the inner margin of the hand. It is used in hollowing out the palm.
The lumbricales are four in number, and arise from the radial sides of the tendons of the flexor profundus. They terminate in little flat tendons, which are inserted into the tendinous expansion of the extensor communis on the back of the first phalanx of each finger; they serve to bend the first phalanges.
The interosseous muscles, seven in number, fill up the interstices of the metacarpal bones; four belong to the palm, and three to the back of the hand. They arise from the base and sides of the metacarpal bones, and are inserted into the sides of the first phalanges, and into the tendinous membrane on the back part of the fingers. The palmar are the prior indicis, the posterior indicis, the prior annularis, and the interosseus digiti auricularis. The dorsal are the prior medii, the posterior medii, and the posterior annularis.
Pl. 124, fig. 15 17, deltoides; 18, pectoralis major; 19, biceps; 20, pronator teres; 21, flexor sublimis digitorum; 22, supinator longus; 23, flexor carpi radialis. Fig. 16 5, deltoides; 7, triceps; 8, extensor digiti minimi; 9, extensor carpi ulnaris; 10, extensor communis digitorum; 11, abductor pollicis longus; 12, extensor pollicis brevis; 13, extensor pollicis longus; 14, external interosseous muscles; 15, tendons of the extensor communis digitorum. Fig. 174, deltoides.
Pl. 125, fig. 19 15, biceps; 16, flexor digitorum communis sublimis; 17, extensor pollicis longus. Fig. 20 6, supra-spinatus; 7, infra-spin atus; 8, teres minor; 16, triceps extensor cubiti; 17, brachialis internus; 18, anconæus; 19, extensor carpi radialis; 20, flexor carpi ulnaris; 21, extensor pollicis longus; 22, indicator; 23, abductor pollicis longus; 24, extensor pollicis brevis.
Pl. 126, fig. 20 8, coraco-brachialis; 9, biceps; 10, flexor digitorum profundus; 11, flexor pollicis longus. Fig. 21 14, anconæus; 15, 16, exterior carpi radialis longus et brevis.
Pl. 127, fig. 12 1, supra-spinatus; 2, infra-spiuatus; 3, teres minor; 4, teres major; 5, end of latissimus dorsi. Fig. 13 1, subscapularis; 2, biceps; 3, coraco-brachialis; 4, brachialis internus; 6, teres major. Fig. 14 1, tendon of the triceps; 2, brachialis internus. Fig. 15 1, deltoid; 2, common tendon of the triceps; 3, 4, 5, the long, the external, and the internal portions; 6, anconseus.
Pl. 128, fig. 4 1, pronator teres; 2, flexor carpi radialis; 3, palmaris longus; 4, flexor carpi ulnaris; 5, supinator longus; 6, flexor digitorum communis. Fig. 5 1, flexor digitorum communis sublimis; 2, slit for the passage of the flexor profundus; 3, supinator longus; 4, lower part of the brachialis internus; 5, tendon of the biceps; 6, palmar ligament. Fig. 6 1, flexor communis digitorum profundus; 2, 3, flexor pollicis longus; 4, pronator quadratus; 5 and 6, supinator longus et brevis. Fig. 7 1, extensor digitorum communis; 2, extensor digiti minimi; 3, extensor carpi ulnaris; 4, anconseus; 5, extensor carpi radialis longus et brevis; 6, annular ligament. Fig. 8 1, supinator brevis; 2, anconæus reflected; 3, abductor longus pollicis; 4, extensor pollicis brevis; 5, extensor pollicis longus; 6, extensor indicis. Fig. 9 1, tendon of the extensor pollicis longus; 2, tendon of the palmaris, longus; 3, tendon of the flexor carpi ulnaris; 4, abductor pollicis brevis; 5, opponens pollicis; 6, flexor pollicis brevis; 7, abductor pollicis; 8, palmaris brevis; 9, abductor digiti minimi; 10, flexor brevis digiti minimi; 11, opponens digiti minimi; 12, internal interosseous muscle. Fig. 10 1, 2, 3, external interosseous muscles.
Muscles of the Inferior Extremities
Each inferior extremity is connected to the trunk by the strong ligaments of the hip joint, and by several muscles which pass from the pelvis to the thigh and leg. The muscles of the lower extremities may be conveniently classed into those of the pelvis or hip joint, thigh, leg, and foot; those of the thigh are arranged into posterior, anterior, external, and internal.
1. Muscles of the Hip. These are nine in number: the three glutæi, the pyriformis, the gemini, the two obturators, and the quadratus femoris.
Glutceus maximus covers the greater part of the pelvis, also the upper part of the thigh; it is somewhat square, with the inferior edge thick and round, and covered by a great quantity of fat; this forms the fold of the nates. It arises from the posterior fifth of the crest of the ilium, from the rough surface between the crest and the superior semicircular ridge, of this bone, from the posterior surface of the sacrum, and from the sides of the coccyx. The flat and thick tendon of this muscle is inserted into a rough ridge, which leads from the trochanter to the linea aspera; also into the upper third of that line, and into the fascia lata. Use: to extend the thigh, to abduct and rotate it outwards, and to support and extend the pelvis and the trunk on the lower extremity.
Glutceits medius, triangular, and thinner than the last, arises from the three anterior fourths of the outer edge of the crest of the ilium, and from the surface of the ilium, and is inserted into the upper and outer part of the great trochanter, being also attached anteriorly to the tendon of the glutaeus maximus. Use: to abduct and rotate the thigh, and to maintain the pelvis in equilibrium on the femur.
Glutceus minimus arises from the inferior semicircular ridge on the dorsum of the ilium, and from the rough surface between it and the edge of the acetabulum. The fibres converge and end in a strong, round, twisted tendon, which is inserted into the upper and anterior part of the great trochanter. Use: similar to the last. It also strengthens the ilio-femoral articulation.
Pyriformis is a flattened triangular muscle, the base at the sacrum within the pelvis, the apex at the trochanter. It arises within the pelvis, and is inserted into the upper part of the digital fossa at the root of the great trochanter. Use: to abduct the thigh, to extend and rotate it outwards.
Gemelli, two smaller muscles, placed behind the ilio-femoral articulation, between the ischium and trochanter. The superior arises from the spine of the ischium, and is inserted into the upper part of the digital fossa of the great trochanter. The inferior arises from the upper part of the tuber ischii, and is also inserted into the digital fossa. Use: to rotate the thigh outwards and to abduct it.
Obturator internus is situated partly within the pelvis and partly behind the ilio-femoral articulation. It arises within the pelvis from the superior surface of the thyroid ligament and from the circumference of the thyroid foramen, and is inserted into the digital fossa of the great trochanter. Use: to abduct and rotate the thigh outwards; also to act on the capsular ligament.
Quadratus femoris arises from the external surface of the tuber ischii, anterior to the tendon of the semi-membranosus. It is inserted into the inferior and posterior part of the great trochanter, and into the posterior inter-trochanteric line. Use: to abduct and rotate the thigh outwards.
Obturalor externus, situated at the upper, posterior, and internal portion of the thigh, arises from the inferior surface of the thyroid or obturator ligament, and from the surrounding sarfaces of the pubes and ischium. It is inserted into the lower part of the digital fossa. Use: to adduct the thigh and rotate it outwards.
2. Muscles of the fore part and sides of the Thigh. These are eleven in number.
Tensor vagince femoris arises from the exterior internal part of the anterior superior spinous process and crest of the ilium, and is inserted into a duplicature of the fascia lata on the outside of the thigh, about three or four inches below the great trochanter. Use: to make tense the fascia, to compress the vastus externus, to rotate the thigh inwards, and to assist in flexing and abducting it.
Sartorius, or the tailor’s muscle, is the longest muscle in the body. Thin and flat, like a ribbon, it is situated obliquely along the anterior and inner side of the thigh, arising from the anterior superior spine of the ilium and from the notch below that process. It extends obliquely across the thigh to its inner side, and descending perpendicularly to the knee, it passes behind the condyle of the femur. It then turns forwards and outwards towards the inner side of the upper end of the tibia, into which it is inserted below the tubercle. Use: to flex the leg on the thigh and the thigh on the pelvis, to cross the lower extremities, &c.
Rectus femoris is a long and flat muscle, placed vertically on the fore part of the thigh. It arises by two tendons, one from the anterior inferior spinous process of the ilium, the other from the superior and external border of the acetabulum. These soon unite into a strong fleshy belly ending in a flat tendon, which is inserted into the upper edge of the patella. Use: to extend the leg on the thigh and to flex the leg on the pelvis. Its action is greatly facilitated by the patella, which enables it to act at greater mechanical advantage. This muscle is internally united to three others subjacent to it; the four, in fact, form a single quadriceps muscle. Of these the external is called vastus externus, the middle, crarus, and the internal, vastus internus.
The vastus externus arises from the root and anterior part of the great trocha,nter, from the outer edge of the linea aspera, and from the oblique ridge which leads to the external condyle. It is inserted into the external surface of the tendon of the rectus, and into the patella. It extends the knee, and rotates the leg outwards.
Vastus internus arises on the anterior edge of the femur, and is inserted into the inner edge of the tendon of the rectus and into the patella. Use: to extend the knee and turn the leg a little inwards.
Crurceus, between the two last, arises from the anterior and external part of the femur, and is inserted into the upper and anterior edge of the patella. It assists the vasti and rectus in extending the leg.
Gracilis, situated at the inner side of the thigh, beneath the integuments and fasciæ, arises from the lower half of the symphysis and from the inner edge of the descending ramus of the pubes. It is inserted into the superior part of the internal surface of the tibia. Use: to abduct the leg and thigh, to bend the knee, and turn the leg and foot inwards.
Pectinæus arises from the linea innominata and the convex surface below it on the horizontal ramus of the pubes, and is inserted into the rough ridge leading from the lesser trochanter to the linea aspera. Use: to adduct and flex the thigh and to rotate it inwards.
Triceps adductor femoris consists of the three following portions, which pass in distinct laminæ from the pelvis to the thigh:
Adductor longus, flat and triangular, situated at the upper and internal part of the thigh, arising from the anterior surface of the pubes, and inserted into the middle third of the linea aspera.
Adductor brevis, arising from the anterior inferior surface of the pubes, and inserted into the superior third of the internal root of the linea aspera.
Adductor magnus, the largest and longest of the three, arising from the anterior surface of the descending ramus of the pubes, and from the ramus of the ischium, and inserted into the rough ridge leading from the great trochanter to the linea aspera. The three adductors, in addition to adducting the limb, can rotate it outwards. They also serve to support and steady the pelvis on the thigh; likewise to flex and extend the thigh on the pelvis.
3. Muscles of the back part of the Thigh. They are only three in number, and are commonly called hamstrings; the semi-tendinosus and, semi-membranosus form the inner, the biceps the outer hamstring.
Biceps flexor cruris consists of a long and a short head. The former arises from the outer and back part of the tuber ischii in common with the semi-tendinosus, and about the inferior third of the thigh it joins the short head which arises from the linea aspera. The tendon of the common muscle descends behind the knee, then turning forwards and outwards, is inserted into the head of the fibula. Use: to flex the knee joint, to extend the thigh, and rotate the limb outwards. It also assists in raising the body when bent in, and in maintaining the erect posture.
Semi-tendinosus arises from the tuberosity of the ischium, and is inserted into the anterior angle of the tibia below its tubercle. Use: to flex the knee, and rotate the leg inwards; also to extend the thigh, to support the pelvis, and prevent the trunk from bending forwards.
Semi-membranosus, beneath the preceding, arises from the upper and outer part of the tuber ischii, and descending ends in a tendon, which passes behind the internal condyle and divides into three processes. The first is inserted into the external condyle of the femur; the second is inserted into the posterior part of the tibia and fibula, and is also continuous with the deep fascia of the leg; the third is inserted into the head of the tibia. Use: to extend the thigh on the leg, to flex and rotate the knee, and to strengthen the back part of the joint.
4. Muscles of the anterior and external part of the Leg. The muscles on the fore part of the leg are four in number, viz. the tibialis anticus, extensor pollicis, extensor communis digitorum, and peronaeus tertius. Those on the outer side of the leg are the peronaeus longus and brevis.
Tibialis anticus, on the outer side and next to the tibia, arises from the outer part of the superior two thirds of the tibia, from the head of the fibula, and from the interosseous ligament; it is inserted into the inner side of the great or internal cuneiform bone, as also into the base of the great toe. Use: to flex the ankle, to add act the foot, to turn the toes inwards, and to support the leg when standing.
Extensor digitorum longus arises from the external part of the head of the tibia, and from the upper part of the fibula, and is inserted by four tendons into the back of the last phalanx of each toe (except the great toe). Use: to extend the toes and flex the ankle.
Extensor pollicis proprias arises from the inner edge of the middle third of the fibula, and is inserted by two tendinous fasciculi, one into the base of the first phalanx, and the other into the base of the second or last phalanx of the great toe. Use: to extend the great toe and flex the ankle.
Peronceits tertius or anticus arises from the anterior surface of the lower half of the fibula, and is inserted into the base of the fifth metatarsal bone. Use: to extend the little toe, to flex the ankle, and to raise the outer edge of the foot.
Peronæus longus arises from the head of the fibula and from the adjacent surface of the tibia; it is inserted into the outer side of the metatarsal bone of the great toe and into the adjacant sesamoid bone. Use: to extend the ankle joint, to press the great toe against the ground as in walking, and to turn the foot outwards.
Peronæus brevis arises from the lower half of the fibula, and is inserted into the base of the metatarsal bone of the little toe and into the os cuboides. It is similar to the last in its uses.
5. Muscles of the back part of the Leg. These are seven in number, arranged in a superficial and a deep layer; the former consists of the gastrocnemius, soælus, and plantaris; the latter, of the tibialis posticus, flexor pollicis longus, flexor digitorum communis, and poplitseus.
Gastrocnemius arises by two heads, one from a digital depression on the upper and back part of the internal condyle of the femur, the other from above the external condyle. The two fleshy bellies form the calf of the leg, these ending in a broad flat tendon about the middle of the limb, which with the tendon of the subjacent solseus is inserted into the lower and back part of the os calcis, as the tendo achillis. Use: to extend the ankle joint, and to throw the whole weight of the body forward on the. toes, as in progression.
Plantaris arises from the back part of the femur, above the external condyle and from the posterior ligament of the knee; it is inserted into the os calcis a little anterior to the tendo achillis. Use: to extend the foot and turn it inwards; also to flex the knee.
Solæus arises from the back part of the tibia and fibula by two slightly developed heads, and is inserted into the. os calcis by the tendo achillis, common to it and the gastrocnemius. It assists in extending the ankle, but can exert no influence on the knee joint.
Poplitæus arises from a depression on the external surfface of the outer condyle, and is inserted into a flat triangular surface which occupies the superior fifth of the posterior surface of the tibia. Use: to bend the knee, and when bent to twist the foot inwards.
Flexor digitorum perforans arises from the posterior flat surface of the tibia, and is inserted bj four tendons into the base of the last phalanx of each of the four lesser toes. Use: to flex the metatarsus and all the phalanges of the toes.
Tibialis posticus arises from the posterior and internal part of the fibula, and is inserted into a tuberosity on the inferior and internal part of the os naviculare. Use: to extend the ankle, and to raise the inner edge of the foot from the ground.
Flexor pollicis longus arises mainly from the two inferior thirds of the fibula, and is inserted into the base of the last phalanx of the great toe. Use: to flex this toe, to extend the ankle, and to adduct the foot.
6. Muscles of the Foot. There is but one muscle in the upper surface of the foot, the extensor digitorum brevis. Those in the sole of the foot are very numerous, and may be divided into four laminæ. The muscles of the first lamina are, the abductor pollicis, flexor digitorum brevis, and abductor minimi digiti; in the second layer are the long flexor tendons, the accessory muscle, and the lumbricalis. The third layer consists of the flexor pollicis brevis, adductor pollicis, transversalis pedis, and flexor minimi digiti. In the fourth are the interosseous and the tendon of the peronseus longus.
Extensor digitorum brevis arises from the upper part of the os calcis, from the cuboid bone, the astragalus, and the annular ligament; it ends in four tendons, which are inserted into the upper part of all the four large toes. It serves to extend the toes and to rotate the anterior part of the foot outwards.
Abductor pollicis arises mainly from the inner part of the os calcis, and is inserted into the internal sesamoid bone, and into the internal side of the first phalanx of the great toe. It serves to flex the great toe and to separate it from the rest.
Flexor digitorum brevis perforatus arises from the inferior and internal part of the os calcis, and about the middle of the foot divides into four muscles, each ending in tendons. Each tendon is perforated by the long flexor tendon, and is ultimately inserted into the lateral borders of the second phalanges. It assists to preserve the arch of the foot, and helps the long flexor muscle.
Abductor minimi digiti arises principally from the outer side of the os calcis, and is inserted into the outer side of the base of the first phalanx of the little toe and into the adjoining surface of the metatarsal bones. It flexes the little toe and separates it from the others.
Accessorius arises bifurcated from the inferior and lateral borders of the OS calcis, and is inserted into the upper and outer part of the tendon of the flexor digitorum longus just before it divides. It assists the long flexor, and counteracts its obliquity.
Lumbricales are four small muscles which arise from the angles between the tendons of the flexor digitorum longus; each is inserted into the internal side of the first phalanx of the four toes, there being none for the great toe. They adduct and assist in flexing the four toes.
Flexor pollicis brevis arises from the anterior inferior part of the os calcis, and from the cuboid and external cuneiform bone, and passing forwards is divided into two tendons inserted into the sesamoid bones beneath the first phalanx of the great toe. It flexes the first joint of the great toe, and approximates this toe to the others.
Adductor pollicis arises from the calcaneo-cuboid ligament and from the base of the second, third, and fourth metatarsal bones; it is inserted into the external sesamoid bone. It draws the great toe outwards towards the others, and flexes it so as to bring it beneath them.
Transversalis pedis arises by distinct slips from the anterior extremities of the four external metatarsal bones. It is inserted into the external sesamoid bone of the great toe along with the last mentioned. It approximates the toes and contracts the arch of the foot.
Flexor brevis minimi digiti arises from the cuboid and fifth metatarsal bones, and is inserted into the inner side of the base of the first phalanx of the little toe, which it serves to flex and adduct.
The interossei muscles are seven in number; three are seen on the sole and four on the dorsum. The inferior are adductor medii digiti, adductor quarti digiti, and adductor minimi digiti. They arise from between the metatarsal bones of the four external toes, and are inserted into the inner side of the base of the first phalanx of the three lesser toes. The superior interossei are all abductors, viz. internus digiti secundi, externus digiti secundi, abductor digiti medii, and abductor digiti quarti.
Pl. 124, fig. 15 29, tensor vaginæ femoris; 30, pectinaeus; 31, sartorius; 32, gracilis; 33, rectus femoris; 34, ligamentum patellæ; 35, extensor digitorum communis; 36, tibialis anticus. Fig. 16 17, giutæus maximus; 18, gracilis; 19, vastus externus; 20, biceps flexor cruris; 21, gastrocnemius.
Pl. 125, fig. 19 28, extremity of the psoas and iliacus externus; 29, adductor brevis; 30, adductor longus; 31, cruræus; 32, vastus externus; 33, vastus internus; 34, extensor digitorum communis; 35, extensor longus pollicis. Fig. 20 31, plantaris; 32, solæus; 33, tendon of the gastrocnemius.
Pl. 126, fig. 20 19, quadratus lumborum; 20, psoas parvus; 21, psoas magnus; 22, iliacus internus; 23, adductor brevis; 24, adductor longus; 25, adductor magnus; 26, gracilis. Fig. 21 26, glutæus minimus; 27, obturator internus; 28, obturator externus; 29, adductor magnus; 31, poplitaeus; 32, flexor digitorum communis; 33, flexor pollicis longus; 34, peronæus longus; 35, peronæus brevis; 36, 37, tibialis posticus.
Pl. 128, fig. 11 1, glutæus maximus; 2, glutæus medius. Fig. 12 1, glutæus medius; 2, pyriformis; 3, tendon of the obturator internus; 4, quadratus femoris; 5, section of the tendon of the glutæus maximus. Fig. 13 1, section of the pyriformis; 2, glutæus minimus; 3, obturator internus; 4, quadratus femoris; 5, adductor femoris; 6, biceps flexor cruris; 7, semi-tendinosus; 8, semi-membranosus. Fig. 14 1, psoas magnus; 2, iliacus internus (both in section); 3, sartorius; 4, tensor vaginæ femoris; 5, rectus; 6, vastus externus; 7, pectinæus; 8, adductor longus; 9, gracilis. Fig. 15 1, the four extensors of the leg, the rectus supposed to be cut off: 2, adductor brevis; 3, adductor magnus; 4, obturator externus. Fig. 16 1, tibialis anticus; 2, extensor pollicis longus; 3, extensor digitorum communis; 4 and 9, peronæus longus; 5 and 8, peronæus brevis; 6, extensor communis brevis; 3′ and 7, peronæus tertius; 10, annular ligament on the back of the foot. Fig. 17 1, flexor digitorum brevis; 2, abductor pollicis; 3, flexor pollicis brevis; 4, abductor digiti minimi; 5, flexor brevis digiti minimi. Fig. 18 1, flexor pollicis brevis; 2, adductor pollicis; 3, transversalis plantaris; 4, tendon of the peronseus longus. Fig. 19 interosseous muscles of the back of the foot.
![]() The Vascular System (Angeiology)
The Vascular System (Angeiology)
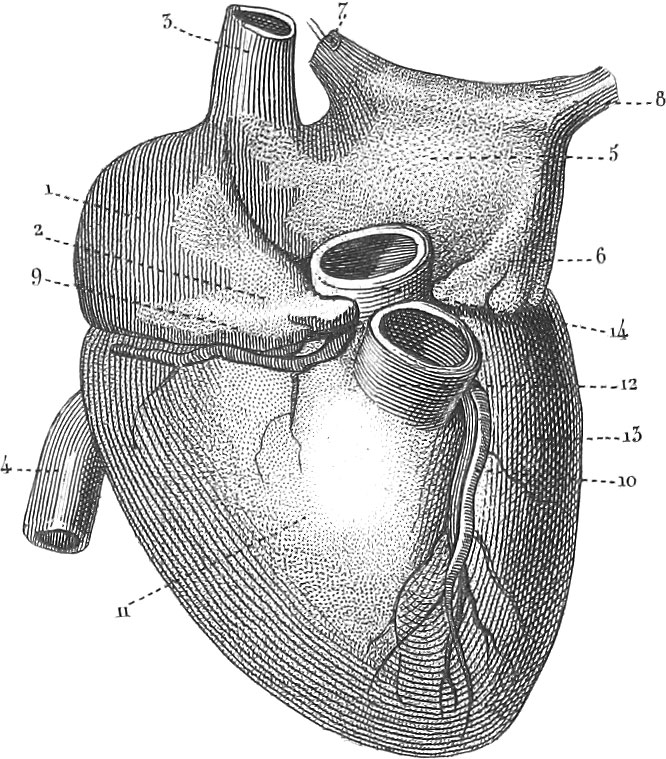 The Vascular System (Angeiology)
The Vascular System (Angeiology)The Vascular System consists of membranous ramifying tubes, which conduct either blood or fluids to be added to the blood for the sake of restoring to it the materials necessary for its normal functions. The blood, from which is derived the material of life and growth, is furnished by the food taken into the stomach, which after undergoing certain operations, subsequently to be explained, and after being strained through exceedingly fine tubes called lacteals, is introduced into the general circulation by the thoracic duct. The blood circulates through all parts of the body mainly by the impulsion of a central engine, the heart, which continues pulsating at regular intervals during the entire life of the animal. Vessels which conduct blood from the heart are known as arteries, while those which bring it back again are veins. The former are distinguishable from the latter by their exhibiting the phenomena of pulse. The arteries pass to all parts of the body, dividing and subdividing continually as they recede from the heart, until finally they end in ramifications so fine as only to be appreciable by the microscope. These terminal branches are called capillaries. The capillaries are continued into the veins, which present an appearance much like that of the arteries, viz. a tree excessively ramifying, with the trunk resting on the heart, and the branches ending in the capillaries, which latter thus constitute the peripherical medium of communication between the arteries and the veins. The blood proceeds from the heart through the arteries to the capillaries, where it undergoes certain changes; passing into the veins from these, it again reaches the heart, thus performing a round known as the circulation of the blood. The nutritious particles of the blood pass through the thin walls of the capillaries into the various tissues, for the sake of supplying the wear and tear of animal life; the dead or effete portions are taken up in the state of lymph by another set of vessels called lymphatics, which discharge their contents into the veins, ultimately to be subjected to certain influences which prepare them for again playing their part in the general circulation. The chyliferous system is closely allied to the lymphatic. This consists of excessively minute canals, which extend from the intestines to the thoracic duct, and are called lacteals, on account of their white appearance when distended with the milk-like chyle.
The blood, when returned from the capillaries through the veins, is no longer fit for the purposes of life, and must accordingly be purified, or freed from the dead matters with which it is loaded. This purification is mainly effected through the instrumentality of the lungs, in which the venous blood comes in contact with the atmosphere and constitutes respiration. In the lungs, the oxygen of the air is absorbed by the blood, and uniting with the superabundant carbon, forms carbonic acid, which, as a gas, may be exhaled. The accession of oxygen converts the dark venous blood into the bright red arterial, which again returning to the heart, is impelled into the arteries as before. This union of the carbon of the blood with oxygen absorbed from the air, takes place not only in the lungs but in the bloodvessels. The circulation of the blood through the arteries, capillaries, and veins, is known as the greater or systematic circulation, that through the lungs being the lesser or pulmonic.
Special Anatomy of the Heart
The central organ of the vascular system, the heart, is a hollow, irregularly conical body, slightly flattened posteriorly, and so situated in the thoracic cavity between the two lungs, as that its base from which the blood-vessels arise is superior, and the apex directed downwards and to the left.
The heart does not lie loose in the thorax, but is inclosed in a membranous bag called the pericardium. The external or fibrous layer is closely united to the pleura or lining membrane of the thorax, and to the mediastinum, a nearly vertical partition formed by the juxtaposition of the pleuræ of opposite sides. Although, on the whole, of similar shape to the heart, it is yet inverted, the apex being superior and the base inferior. Below it is firmly united to the tendon of the diaphragm. It consists essentially of two layers, an external or fibrous, and an internal or serous. The serous layer is reflected over the heart, and secretes a thin yellowish fluid, the liquor pericardii, which lubricates the heart, and permits it to play freely: within its pericardium. The amount of this liquor when in health seldom exceeds a teaspoonful.
The heart is a strong muscular bag, divided into two compartments, two auricles and two ventricles. On looking at it from before, there will be seen a longitudinal farrow, sulcus longitudinalis, which divides it into right and left portions; this farrow corresponds to the internal partition dividing the right auricle and ventricle from the left auricle and ventricle. A second furrow, sulcus transverscalis or coronalis, intersects the first at right angles, and marks the partition between the right and left auricle and the right and left ventricle. The two auricles form the base of the heart, the ventricles constituting its body; and the anterior end of the left ventricle, by being extended somewhat beyond the right, forms the apex. The auricles are in immediate connexion with the great venous trunks; the right with the two venæ cavæ, the left with the pulmonary veins, all of which conduct blood to the heart.
The interior of the heart is provided with a serous layer or membrane, as well as the exterior. This, which is known as the endocardium, not only constitutes a smooth lining to the cavities of the heart, and thus greatly facilitates the passage of the blood, but, by its duplicatures, it forms the valves which are situated in the openings in the heart, and regulate the proper flow of the blood. Starting from the entrance of the two venæ cavæ, it enters the right auricle, and there forms the eustachian and coronary valves; passing through the opening between the right auricle and ventricle, it increases in density, and forms the loose pendulous tricuspid valve. Approaching the orifice of the pulmonary artery, it assists in forming the sigmoid valves, and becomes continued into the lining internal coat of that vessel and its ramifications. In like manner, through the left cavities of the heart we can trace it from the pulmonary veins into the left auricle, thence into the left ventricle and aorta, forming in its course the mitral and semilunar valves.
On removing the serous investment of the exterior of the heart, we come to the muscular tissue, which will be seen to be much thicker over the ventricles than over the auricles, and over the left ventricle than over the right.
Considering, in the next place, the individual cavities of the heart, we commence with the right auricle. This constitutes an oblong cuboidal cavity, joined at its posterior superior angle by the descending vena cava, and at its posterior inferior angle by the ascending vena cava. The structure of the auricle between these two points appears to be only a continuation of that of the veins. In front of this continuation of the two veins the auricle is dilated into a pouch, called its sinus, the upper extremity of which is elongated into a process with indented edges, somewhat resembling the ear of an animal, whence the term auricle. About midway between the orifices of the two vense cavse is seen a transverse prominence, the tuherculum Loveri. This cavity is separated from the left auricle by a thin partition common to the two auricles. On the septum or partition, below its middle, is a superficial circular depression, the fossa ovalis, surrounded by an elevated margin, called the annulus. In the fœtus, before birth, this fossa is occupied by a hole, foramen ovale, through which the blood passes directly from the right to the left auricle, without first going through the lungs.
Just below the fossa ovalis is seen the Eustachian valve, which in the fœtus serves to direct the blood to the foramen ovale; in the adult it appears to oppose the reflux of blood into the ascending vena cava at the lower part of the right auricle; to the left of the Eustachian valve is seen the orifice of the large coronary vein of the heart, protected by a small semilunar valve, valvula Thebesii. Between the right auricle and ventricle is a round hole, about an inch in diameter, called the ostium venosum, or right auriculo-ventricular opening, for the passage of the blood. This is surrounded by a dense white line, designated as the right tendon of the heart.
The walls of the right auricle are formed by muscular fibres. On the sinus these are collected into small transverse fasciculi, called musculi pectinati, which leave between them deep interstices, in which the external and internal membranes of the heart come in contact.
The right ventricle. This forms the greater part of the anterior surface of the heart, and is separated posteriorly from the left ventricle by a thick septum. The internal surface of the cavity of the right ventricle is covered by muscular fasciculi, known as the columnæ carneæ, some of them passing from one side to the other, and others contributing to the valvular arrangement between the right auricle and ventricle. These, called chordæ tendineæ, pass to the edge of the tricuspid valve, which arises from around the margins of the ostium, and projects into the cavity of the ventricle.
The opening for the pulmonary artery is situated above the ostium venosum. It is round, and about an inch in diameter, and furnished with three valves, called semilunar and sigmoid, which are capable of completely closing this orifice, should the blood flow back from the pulmonary artery, but which lie close pressed to the sides when the current is in its normal direction. Through the pulmonary artery venous blood is carried to the lungs.
The blood, after circulating through the lungs, is returned by the pulmonary veins into the left auricle, at the anterior inferior side of which is seen the left auriculo-ventricular opening, or the communication with the left ventricle, about an inch in diameter. This, like the right auricle, is constituted by a sinus venosus and auricular appendage.
The left ventricle constitutes the principal bulk of the heart, and its walls are nearly three times as thick as those of the right ventricle. Its internal surface is roughened by the same columnæ carneas as the right. The ostium venosum, or opening between the left ventricle and auricle, is on the side also fortified by a valvular arrangement, the mitral valve, which prevents the reflux of blood. It is retained in the left ventricular cavity by chordæ tendineæ. Close to the ostium is the opening for the aorta, guarded by three semilunar valves, very similar in arrangement to those of the pulmonary artery, being, however, stronger.
Passage of blood through the heart. By the alternate contraction and dilation of the different chambers of the heart, the blood is caused to circulate through it and the bloodvessels proceeding from it. The right and left ventricles contract, while the two auricles expand, and vice versâ; contraction of the ventricles being known as the systole, and their dilation the diastole. Commencing with the right side of the heart, we find that when the auricle contracts, the blood is forced towards the auriculo ventricular opening, and backwards into the venæ cavæ. The simultaneous expansion of the right ventricle, however, affords a free passage for the blood from the right auricle, which accordingly rushes through the ostium. The ventricle now contracting, forces the blood towards the ostium, and towards the pulmonary artery. Through the former it cannot pass, by reason of the tricuspid valve; and as the semilunar valves at the entrance of the pulmonary artery afford no impediment, the blood is drawn into the lungs. Simultaneously with this contraction of the ventricles, the right auricle dilates and becomes filled with fresh venous blood from the venæ cavæ. The blood, after passing through the lungs, is brought back to the left auricle, which, contracting at the moment when the left ventricle is expanding, forces the blood into the left ventricle. The contraction of this ventricle drives the blood into the aorta, its reflux into the auricle being prevented by the mitral valve. The semilunar valves of the pulmonary artery and aorta prevent the reflux of blood into their respective ventricles.
Pl. 130, fig. 1, right half of the heart from before: 1, right auricle; 2, right ventricle. Fig. 2, left half of the heart from before: 1, left auricle; 2, left ventricle. Fig. 4, larynx, trachea, pericardium, and lungs: 5, pericardium. Fig. 5, heart from before: 1, right sinus; 2, right auricular appendage (the two constituting the auricle); 3, superior vena cava; 4, inferior vena cava; 5, 6, left sinus and appendage, or left auricle; 7, 8, pulmonary veins; 9, sulcus transversalis; 10, longitudinal furrow or fissure; 11, right ventricle; 12, pulmonary artery; 13, left ventricle; 14, aorta. Fig. 6, section of the right half of the heart: 1, right auricle; 2, fossa ovalis; 3, Eustachian valve; 4, opening of the great coronary vein with the valvula Thebesii; 5, right ventricle with its columnæ carneæ; 6, a point of the tricuspid valve with the chordæ tendineæ; 7, pulmonary artery with two of the semilunar valves. Fig. 7, section of the left half of the heart: 1, left auricle with the openings of the pulmonary veins; 2, left ventricle; 3, mitral valves; 4, aorta with two semilunar valves. Fig. 8, direction of the muscular fibres of the heart: 1, 2, 3, fibres of the auricles; 4, fibres of the ventricles; 5, openings for the large vessels of the heart; 6, place where the fibres twist round each other at the apex, to become united with the deep layers; 7, place where the superficial anterior and posterior fibres interlace and become united with the deep fibres; 8, 9, openings of the pulmonary artery and aorta.
Special Anatomy of the Arteries
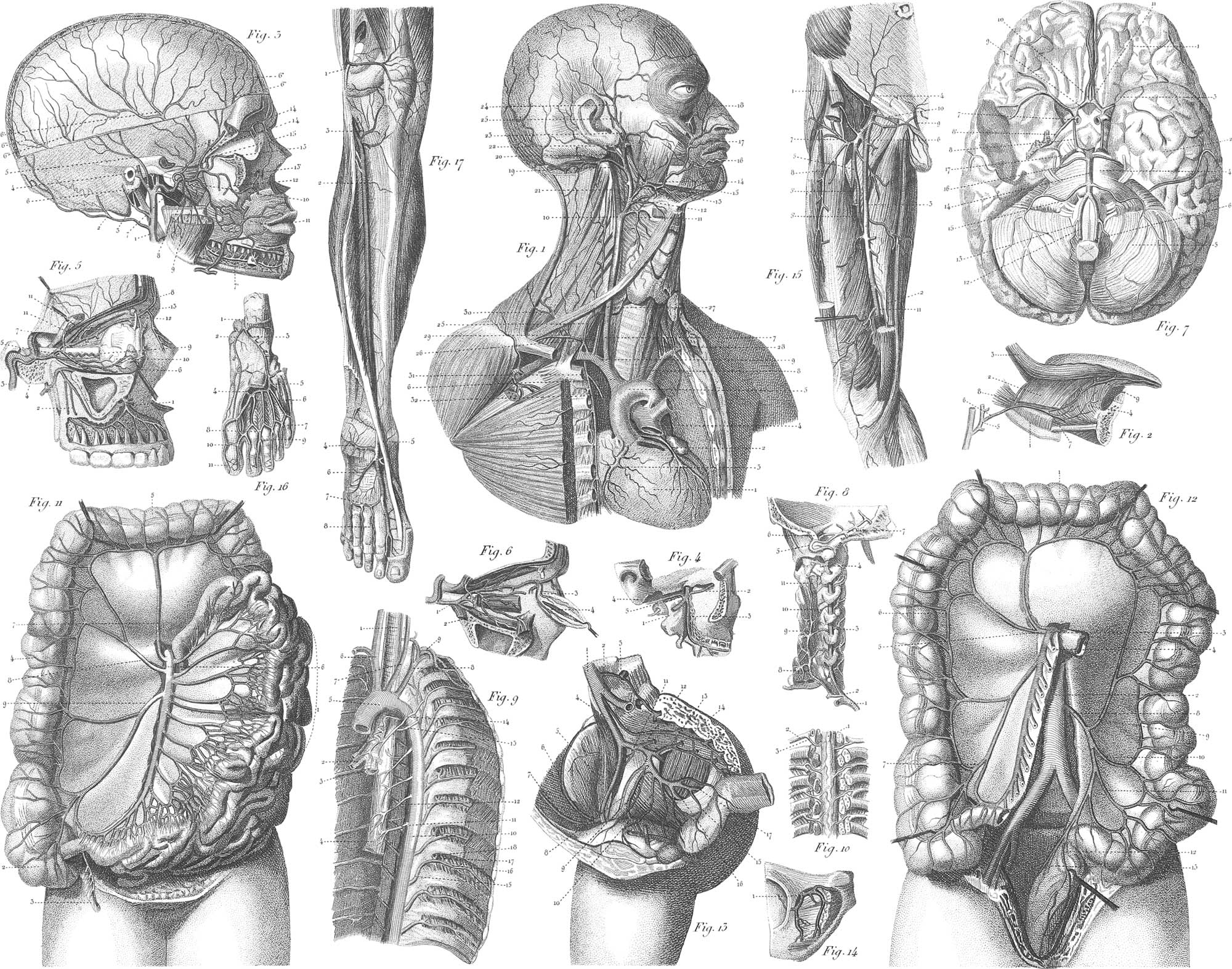
The aorta, situated on the base of the heart, may be considered as the main trunk of a tree, whose ramifications ever increasing constitute the arteries, the ultimate branches being the capillaries. The various arterial divisions are named partly from their regional situation, as subclavian, axillary, &c., partly from their relative position, as deep or superficial, and partly from their distinction, as cerebral, ophthalmic, &c. The names “aorta” and “artery” show the opinion entertained by the ancients with respect to their functions, being supposed to conduct vital air exclusively, from being found empty of blood after death, yet still distended.
The arterial tubes are of a dense structure, and when empty preserve their form without collapsing. They are composed of three principal coats or tissues. The first or external is fibro-cellular, strong and resisting, and connects the vessels with the surrounding parts. The second, or middle, or proper coat of the arteries is thickest, and consists of yellowish and rather dry fibres, elastic but not brittle; although circular they do not form complete rings. By the aid of the microscope, this coat may be divided into three laminæ: an external, thin, elastic, and yellow; a middle, composed of circular fibres similar to those of unstriped involuntary muscle; and an internal, similar to the last, but with the fibres longitudinal. The internal coat of an artery is smooth and polished, and may be subdivided into two laminæ, the internal composed of tesselated epithelium, and resting on a basement membrane with longitudinal and internal fibres. Although the external system is devoid of exact symmetry, yet, with a few exceptions, one description will apply to either side. Arteries are all supplied with nutrient vessels and nerves from the adjacent parts.
The Arch of the Aorta
The aorta, arising from the superior posterior end of the left ventricle, passes beneath the pulmonary artery, and is entirely concealed in front by it. Keeping to the right, it emerges at the base of the heart, between the right auricle and the trunk of the pulmonary artery, being bounded on the right side by the descending vena cava. Continuing its ascent, it forms a curvature with the convexity upwards, the summit of which arises to within about an inch of the superior edge of the sternum. This curvature is in front of the third and fourth dorsal vertebræ, and in its course the aorta passes over the right pulmonary artery, across the left bronchus, and applies itself to the left side of the spine about the third or fourth dorsal vertebra. This bend is known as the aortic arch, arcus aortæ. In its descent down the thorax the aorta is in contact with the left surface of the bodies of the dorsal vertebræ. At the lower part of the thorax, it inclines towards the middle line of the vertebræ in order to reach the hiatus aorticus of the diaphragm, through which it penetrates to the abdomen. Here it descends in front of the lumbar vertebræ, somewhat on their left side, ceasing at the intervertebral space between the fourth and fifth vertebræ by division into two large trunks, the primitive iliacs, one for each lower extremity and the corresponding side of the pelvis. In the course of the aorta from the heart to the loins, it first gives off the branches which supply the heart, then those for the head and superior extremities, then those for the sides of the thorax, and afterwards in the abdomen it detaches the trunks which supply the viscera and sides of the abdomen.
From the arch of the aorta there arise five arteries: the right and left coronary, the innominata, the left carotid, and the left subclavian. Exceptions to this arrangement not unfrequently occur, as in addition to the two coronary there are sometimes but two arteries, sometimes six.
Coronary Arteries. The right and left coronary arteries are the nutrient vessels of the heart. They arise above two of the sigmoid valves, and communicate freely with each other by their ramifications,
The arteria innominata, about an inch and a half in length, arises from the upper part of the arch, at the junction between the ascending and horizontal portion; it ascends obliquely to the right side in front of the trachea and of the right pleura, and opposite to the sternal end of the clavicle divides into the right subclavian and right carotid arteries.
We thus have two pairs of arteries to consider for the head and superior extremities, two of them, the left common carotid and the left subclavian, arising immediately from the arch of the aorta; while the right subclavian and carotid are constituted by the bifurcation of the arteria innominata, about an inch from the aortic arch.
The Cartoid Arteries
The right arises from the innominata, the left from the arch of the aorta; they ascend obliquely outwards as far as the os hyoides, where they divide into an external and an internal.
1. The External Carotid Artery ascends obliquely backwards to the fore part of the meatus auditor! us covered by the skin, platysma, and fascia, as also by the digastric and stylo-hyoid muscles, the parotid gland, and portia dura nerve. It gives off ten arteries in three sets: anteriorly, the superior thyroid, lingual, and labial; posteriorly, the muscular, auricular, and occipital; superiorly, the pharyngeal, transverse, facial, temporal, and internal maxillary.
The superior thyroid arises opposite to the cornu of the thyroid cartilage, and descending obliquely forwards beneath the sterno-thyroid and omohyoid muscles, sends off the following branches: 1, the superficial, distributed to the integument and to the superficial muscles; 2, the laryngeal, to the muscles and mucous membranes of the larynx; 3, hyoidean, to the lower border of the os hyoides and adjacent muscles; 4, superior thyroid, to the thyroid gland.
The lingual artery arises immediately above the preceding; it ascends tortuously forwards and inwards, above the os hyoides to the base of the tongue, between the hyo and genio-hyoglossi muscles, and running horizontally forwards towards the tip of the tongue, gives off the following branches: 1, hyoidean; 2, dorsalis linguæ, which ascends to the dorsum of the tongue and is lost on the mucous membrane near its base, also on the velum and fauces; 3, sublingual, to the sublingual gland, mylo-hyoid muscle, and mucous membrane of the mouth; 4, ranine, the trunk continued along the lingualis muscle to the tip of the tongue.
The labial or external maxillary artery arises opposite the os hyoides, ascends behind the digastricus, and between the submaxillary gland and the base of the jaw, and turning around the latter rises towards the sides of the nose. In the neck it gives off: 1, the inferior palatine to the velum; 2, glandular, to the submaxillary and adjoining lymphatic glands; 3, submental, to the chin and surrounding muscles. On the face it gives off: 4, inferior labial, to the muscles and integuments between the lip and chin; 5, inferior and superior coronary, which run along the borders of the lips; 6, lateralis nasi, to the side of the nose; 7, angularis, which communicates with the ophthalmic.
The muscular artery descends obliquely backwards and divides into several branches, which are principally distributed to the sterno-mastoid and to the surrounding cellular tissue and glands.
The occipital artery arises opposite the labial, ascends obliquely backwards behind the digastric, then curves horizontally backwards between the mastoid process and the atlas, and near the mesial line it ascends on the occiput. It gives off several muscular branches, some to the mastoid and trapezius muscles, several to the deep muscles on the sides and back of the neck; and in the occiput it divides into tortuous branches which ascend in different directions in the scalp, and inosculate with the different arteries in that region.
The posterior auricular artery arises above, often in common with the occipital; it ascends behind the parotid and between the meatus auditorius and the mastoid process; it divides into several branches which are lost in the integument of the ear and in the scalp; one branch, named the stylo-mastoid, enters the foramen of the same name.
The inferior or ascending pharyngeal artery arises near the division of the common carotid, ascends vertically to the base of the skull, and sends off several pharyngeal and palatine branches, ending in a small branch which passes through the foramen lacerum posterius, and supplies the dura mater at the base of the cranium.
The transverse artery of the face arises from the carotid in the parotid gland, and is distributed to the muscles and integument of the face, and joins the branches of the facial artery.
The temporal artery is one of the two terminal branches of the external carotid; ascending over the root of the zygoma, about an inch and a half above the zygomatic arch, it divides into an anterior and posterior branch. The anterior temporal is distributed over the front of the temple and arch of the skull, and anastomoses with its fellow of the opposite side, and with the sapra-orbital and frontal artery. The posterior temporal curves upwards and backwards, and inosculates with the posterior of the opposite side, and with the posterior auricular and occipital artery.
The internal mamillary artery ascends obliquely forwards behind the neck of the maxilla between the pterygoid muscles, and gives off the following branches: 1, the middle artery of the dura mater, which, passing through the foramen spinale of the sphenoid bone, divides into two branches which supply the bones of the cranium and the dura mater; 2, the inferior dental: this passes into the dental foramen and distributes minute arteries to the roots of the teeth. Between the pterygoid muscles it sends off, 3, the deep temporal branches to the temporal muscle; 4, masseteric; 5, pterygoid; 6, buccal, to the cheek; 7, superior dental, to the alveoli and gums; 8, infra-orbital, to the muscles of the face; 9, nasal, to the mucous membrane on the spongy bones and the septum; 10, the superior palatine, to the muscles and mucous membrane of the velum, and to the hard palate; 11, the vidian, a small branch which passes backwards. These terminating branches of the internal maxillary are entangled with the divisions of the superior maxillary.
Pl. 135, fig. 1 1, heart; 2, left, 3, right coronary artery; 4, pulmonary artery cut off; 5, arcus aortæ; 6, arteria innominata; 7, right common carotid; 8, left subclavian; 9, division of the innominata into the right carotid and subclavian; 10, division of the common carotid into outer and inner; 11, superior thyroid; 12, lingual; 13, external niaxillary; 14, inferior or ascending palatine; 15, submental; 16, inferior, and 17, superior coronary arteries of the lips; 18, nasal branch of the angularis; 19, occipital; 20, posterior auricular; 21, ascending pharyngeal; 22, division of the external carotid into two terminal branches; 23, transverse facial; 24, middle temporal; 25, anterior auricular. Fig. 2, the lingual artery; part of the lower jaw removed: 1, os hyoides; 2, hyo-glossus muscle cut away; 3, stylo-glossus muscle; 4, genio-glossus muscle; 5, external carotid; 6, lingual artery; 7, dorsalis linguae; 8, sublingual; 9, ranine. Fig. 3, internal maxillary artery in part; the side of the top of the cranium is supposed to be removed, the ascending ramus of the lower jaw to be sawed off, and the body of the bone deprived of its outer table: 1, external carotid; 2, occipital artery; 3, posterior auricular; 4, superficial temporal; 5, middle temporal; 6, root of the internal maxillary; 6′, middle artery of the dura mater; 6″, 6″, anterior artery of the dura mater; 6‴, 6‴, posterior artery of the dura mater; 7, inferior dental; 7′, its course on the jaw; 8, branches for the pterygoid muscles; 9, for the masseter; 10, for the buccinator; 11, coronary artery of the upper lip; 12, superior dental; 13, infra-orbital at its entrance into, and 13′, at its exit from the infra-orbital canal; 14, 14, deep temporal arteries; 15, entrance of the main trunk into the infra-orbital fissure. Fig. 4, internal maxillary within the fissure: 1, main trunk; 2, infra-orbital artery; 3, superior palatine; 4, vidian.
2. The Internal Carotid Artery ascends along the vertebral column and the side of the pharynx from the common carotid, posterior and external to the external carotid, behind the digastric and styloid muscles, internal to the jugular vein, and anterior to the vagus and sympathetic nerves, to the foramen caroticum in the petrous bone. It then bends tortuously forwards, upwards, and inwards through the carotid canal, enters the cavernous sinus, and passing the anterior clinoid process it divides opposite to the internal extremity of the fissure of Sylvius into its three terminating branches, viz. posterior communicans, anterior cerebri, and media cerebri. In the neck and in the carotid canal it sends off small and unimportant branches; one named tympanic, is distributed to the tympanum through a small hole in the carotid canal. The first branch of any importance is:
The Ophthalmic Artery. This arises close to the anterior clinoid process, and passes through the optic foramen below and external to the optic nerve: in the orbit, it passes round the nerve to the inner side of the cavity and terminates in the inner canthus. While on the outer side of the optic nerve it sends off: 1, centralis retinæ, distributed to the interior of the eye; 2, the lachrymal, which passes along the external rectus muscle and supplies the lachrymal gland and the palpebræ. While above the optic nerve it gives off: 3, the supra-orbital, which passes forwards along the levator palpebræ, and through the superciliary notch, supplying the muscles and integuments of the eyebrow and the scalp; 4, the posterior ciliary, ten or twelve in number and very small, becoming distributed to the choroid coat of the eye; 5, the long ciliary one on each side, passing horizontally forwards as far as the ciliary circle, where they subdivide; 6, muscular arteries to the different muscles in the orbit; 7, ethmoidal, to the mucous membrane in the ethmoidal cells; 8, superior and inferior palpebral to the palpebræ, caruncula, conjunctiva, and lachrymal sac; 9, nasal, to the side of the nose; 10, frontal, to the eyebrow and forehead.
The posterior communicans arises from the carotid opposite to the ophthalmic, passes backwards and inwards, and joins the posterior cerebral circle.
The anterior cerebri, or arteria callosa, passes forwards and inwards above the optic nerve, anastomosing with the opposite by a short transverse branch, the anterior communicans, and ultimately terminates by dividing into branches for the corresponding hemisphere of the cerebrum.
The media cerebri, or middle cerebral artery, passes outwards in the fissure of Sylvius, and divides into two tortuous branches which supply the anterior and middle lobes of the cerebrum, sinking deep in the sulci between the convolutions in the island of Reil.
Pl. 135, fig. 5, distribution of the ophthalmic artery: 1, superior dental; 2, inferior dental; 3, internal carotid; 4, ophthalmic artery; 5, muscular branches; 6, lachrymal; 7, supra-orbital; 8, frontal artery; 9, a short or posterior ciliary; 10, a long Qiliary; 11, 11, ethmoidal; 12, frontal branch. Fig. 6, some of the deep branches of the ophthalmic, the eyeball removed: 1, ophthalmic; 2, artery of the lachrymal sac; 3, superior, and 4, inferior palpebræ. Fig. 7, cerebral arteries: 1, anterior; 2, middle lobe of the cerebrum; 3, fissure of Sylvias; 4, pons varolii; 5, cerebellum; 6, medulla oblongata; 7, section of the trunk of the internal carotid; 8, posterior communicans; 8′, choroid artery; 10, artery of the corpus callosum; 11, anterior communicans.
Subclavian Arteries and Their continuations
The great arterial trunks, of which the subclavian constitute the initial portion, have different names in different parts of their course, the series consisting of the subclavian proper, the axillary, the brachial, and the radial and ulnar.
1. The Subclavian Arteries Proper. The right and left subclavian arteries differ in diameter, length, situation, and relation. The right, as arising from the innominata, is shorter than the left, which springs from the arch of the aorta. The course of each may be divided into three stages: the first extends from the origin to the tracheal edge of the scalenus anticus; the middle stage is the transit of the artery between the soaleni muscles; the third stage extends from those muscles beneath the clavicle to the lower border of the first rib, below which the continued trunk receives the name of axillary artery. In the middle and last stages the right and left arteries are similarly circumstanced in all respects; the first stage is much longer on the left than on the right side.
The right subclavian, in its first stage, passes outwards and a little upwards, having anterior to it the internal jugular and subclavian veins, the sterno-mastoid, hyoid, and thyroid muscles. The left subclavian, from its origin to the scalenus, is nearly vertical, and has anterior to it the sterno-mastoid, hyoid and thyroid muscles, the clavicle and first rib, the left vena innominata, left carotid artery, the left lung and pleura, &c.
The subclavian artery, in the middle stage of its course, on each side of the neck is covered by the sterno-mastoid and anterior scalenus muscle, and lies on the pleura and middle scalenus: the subclavian vein is inferior and anterior.
In the third stage it inclines downwards and outwards, and is covered only by the skin, platysma myoides, fascia, and cellular tissue; it rests on the middle scalenus and the first rib. The vein is inferior and anterior, concealed by the clavicle. The subclavian arteries in their course send off the following branches: vertebral, thyroid axis, internal mammary, superior intercostal, and deep cervical.
The vertebral artery arises from the upper and back part of the subclavian, and, ascending, enters the foramen in the transverse process of the fifth or sixth cervical vertebra, continuing through the corresponding cervical foramina as far as the second vertebra. Bending backwards in an exceedingly tortuous manner, it passes through the foramen in the transverse process of the atlas, and alternately piercing the dura mater, advances within the cranium through the foramen magnum, and unites with the opposite at the lower edge of the pons varolii to form the basilar artery. In this course it gives off small branches to the spinal nerves, and to the intervertebral muscles; at the foramen magnum it gives off, first and second, the posterior and inferior spinal arteries, which descend all along the spinal cord; third, the inferior cerebral artery, which runs tortuously around the medulla oblongata, sending off numerous branches to the inferior surface of the cerebellum.
The basilar artery is formed by the confluence of the two vertebral; it ascends in the median groove on the pons varolii, and at the upper edge of that body divides into four branches, two for each side: first, the superior cerebellar artery, passing backwards to the upper surface of each hemisphere of the cerebellum, in which it spreads its branches; second, the posterior cerebral artery, which receives the posterior branch of the internal carotid, bends backwards and outwards, and spreads its ramifications on the posterior lobe of the cerebral hemisphere. The communication between these posterior cerebral arteries and the posterior branches of the internal carotids, completes that remarkable inosculation known as the circle of Willis; this is formed anteriorly by the two cerebral arteries, with their cross uniting branch; laterally by each internal carotid, and its posterior communicating branch; and posteriorly by the trunk of the basilar, and the roots of the posterior cerebral arteries.
The thyroid axis arises from the upper part of the subclavian close to the scalenus muscle and phrenic nerve; it immediately divides into the four following branches: 1. The inferior thyroid, distributed to the thyroid gland, sending branches also to the trachea, œsophagus, &c.; 2. The ascending cervical, distributed to the anterior scalenus, longus colli, and rectus capitis anticus major muscles; 3. Supra-scapular, which supplies the supra-spinatus and trapezius, as also the infra-spinatus and teres minor; 4. Transversalis colli, which ascending beneath the trapezius, divides into the cervicalis superficialis, going to the superficial muscles of the side and back part of the neck, and the posterior scapular artery.
The internal mammary artery arises opposite the thyroid axis; it descends obliquely forwards, between the cartilages of the ribs and the pleura, as far as the ensiform cartilages; sending off branches to various parts of the thorax, it terminates in the diaphragm and the abdominal muscles.
The superior intercostal artery arises between the scaleni, descends behind the pleura, in front of the neck of the first and second ribs, and supplies the two first pairs of intercostal muscles.
The cervicalis profunda lies opposite to the last, ascends backwards and outwards between the transverse processes of the sixth and seventh cervical vertebræ, and ascending on the back of the neck, supplies the complexus and other deep muscles in that region, and inosculates with the descending branches of the occipital artery.
Pl. 135, fig. 7, arteries of the brain: 12, vertebral artery; 13, posterior inferior cerebellar artery; 14, basilar artery; 15, anterior inferior cerebellar artery; 16, superior cerebellar artery; 17, deep cerebral artery. Fig. 8 1, portion of the subclavian; 2, common trunk of the vertebral and deep cervical arteries; 3, course of the vertebral artery through the transverse processes of the vertebræ; 4, its first curvature; 5, the second curvature or bend; 6, its course within the cranium; 7, basilar artery, with its ramifications; 8, deep cervical; 9, 10, interosculations between this and the vertebral; 11, upper end of the transversalis. Fig. 1 25′, inferior thyroid; 26, vertebral; 27, entrance into the vertebral canal; 28, superior intercostal; 29, transversalis colli; 30, ascending cervical; 31, internal mammary; 32, small branches for the anterior mediastinum.
2. Axillary Artery. This artery descends from the lower edge of the first rib obliquely outwards, to the tendon of the latissimus dorsi muscle; it is covered by the integuments, and at first by the external border of the pectoralis major, still lower down by the tendon only of this muscle; it passes over the first intercostal, serratus magnus, subscapular, and tendons of the latissimus dorsi and teres major. The axillary vein descends along its inner and anterior parts, and the brachial plexus lies posterior and external to it. It sends off the following arteries: thoracica acromialis, superior and long thoracic, the subscapular, the posterior and anterior circumflex.
The acromio-thoracic artery arises from the front of the axillary below the subclavian muscles, above the pectoralis minor, and opposite the fissure between the pectoralis major and deltoid muscles; it divides into several branches, some of which pass to the pectoral muscles, others to the acromion process, deltoid muscle, and integuments of the shoulder and arm. One long brunch accompanies the cephalic vein.
The superior thoracic arises a little below the preceding, sometimes in common with it; it passes forwards and inwards, and divides into branches which supply the cellular membrane and glands in the axilla, the pectoral muscles, the breast and integuments.
The long thoracic artery arises below the lesser pectoral, and, passing obliquely forwards, terminates in the intercostal muscles and integuments.
The subscapular artery arises opposite to and descends along the lower edge of the subscapular muscle, and soon divides into an anterior and a posterior branch; the former supplies the subscapular, serratus magnus, and latissimus dorsi; the latter goes to the infra-spinatus and teres minor muscles.
The posterior circumflex artery arises below the last, and passes out of the axilla to the deltoid muscle.
The anterior circumflex artery is smaller than the preceding, and arises either from it or from the axillary. It sends branches to the deltoid, coraco-brachialis, and biceps; one long branch likewise goes to the synovial membrane of the shoulder joint.
The Brachial Artery descends obliquely outwards to the bend of the elbow, where it divides into the radial and ulnar arteries. It lies on the inner side of the coraco-brachialis and biceps. It is accompanied by a vein on either side, also by the median nerve. In addition to several muscular branches, it sends off the superior and inferior profunda and the anastomotica.
The superior profunda arises below the teres major, and passes downwards between the heads of the triceps and in the musculo-spiral groove of the humerus. It divides into two large branches; one descends in the triceps to the olecranon, the other accompanies the radial nerve to the outer condyle, and communicates with the radial recurrent artery.
The inferior profunda arises opposite to the tendon of the coraco-brachialis, descends on the surface of the triceps, along with the ulnar nerve, to the inner condyle, and communicates with the ulnar recurrent.
Pl. 134, fig. 1, arteries of the axilla and arm: 1, scalenus anticus muscle, behind which lies the axillary artery; 2, the pectoral, and 3, the acromial branch of the thoracico-acromialis; 3, superior thoracic; 4, long thoracic; 5, dorsal branch of the subscapular; 6, subscapular; 7, 8, anterior circumflex; 9, posterior circumflex; 10, brachial artery; 11, profunda; 12, accessory ulnar; 13, radial; 14, recurrent branch of do.; 15, ulnar; 16, anterior; 17, posterior recurrent branch; 18, interosseal artery.
3. The Ulnar Artery is larger than the radial, the other branch of the main trunk of the brachial. It descends along the ulnar side of the forearm to the palm of the hand, covered superiorly by the superficial flexors and pronators, and by the median nerve; inferiorly by the skin and fascia. It passes over the brachialis anticus, flexor profundus, pronator quadratus, the annular ligament of the carpus, and the flexor tendons in the palm of the hand. It is accompanied by two veins and by the ulnar nerve, the latter descending along its ulnar side.
It gives off: 1, the anterior ulnar recurrent, which ascends in front of the inner condyle on the brachialis anticus, and inosculates with the anastomotica; 2, the posterior ulnar recurrent, which ascends behind the inner condyle, and anastomoses with the anastomotica and inferior profunda; 3, the interosseal artery, which passes backwards and divides into an anterior and a posterior branch, the former going to the carpal bones and to the sheaths of the extensor tendons, the latter to the extensor muscles; 4, muscular branches to the two layers of flexor muscles and to the skin; 5, dorsalis carpi ulnaris, to the back part of the wrist and hand; 6, superficial palmar, which forms the palmar arch, bending across the palm of the hand to inosculate with branches of the radial artery; 7, palmaris profundus, which joins the deep palmar branch of the radial artery, thus completing the deep palmar arch.
4. The Radial Artery continues in the direction of the brachial artery, passing along the radial side of the forearm to the wrist; it then turns round the external lateral ligament of this joint, and passes forwards into the palm of the hand, terminating in three branches. It is accompanied by two veins, and the radial nerve is at its external side in the middle of the forearm. It passes over the biceps supinator brevis, pronator teres, flexor digitorum sublimis, flexor pollicis, and pronator quadratus.
It gives off: 1, the radial recurrent to the supinators and extensors, inosculating with the superior profunda; 2, muscular branches, to the flexors and supinators; 3, superficialis volæ, to the small muscles of the thumb, inosculating with the ulnar artery, forming the superficial palmar arch; 4, dorsalis carpi radialis; 5, dorsalis pollicis; 6, radialis indicis; 7, magna pollicis, along the first metacarpal bone, and dividing into two branches; 8, palmaris profunda, which, passing across the metacarpal bones, joins the deep branch of the ulnar, and thus forms the deep palmar arch, from which branches proceed to the interosseal muscles, and to the bones and ligaments of the metacarpus.
Pl. 134, fig. 2, arteries of the forearm and of the palm of the hand: 1, ulnar artery; 2, anterior interosseal; 3, posterior interosseal; 4, superficial palmar; 5, metacarpal branch; 6, 7, digital branches; 8, radial artery; 9, its palmar branch; 10, deep palmar arch; 11, branch to the back of the hand; 12, an anterior branch. Fig. 6, arteries of the lower part of the forearm and the back of the hand: 1, branches of the external interosseal; 2, dorsal branch of the radial; 3, anastomoses on the back of the hand; 4, artery of the thumb; 5, third metacarpal branch.
Thoracic Aorta
The thoracic aorta descends obliquely forwards from the termination of the arch to the diaphragm. It is inclosed in the posterior mediastinum; the root of the left lung above, the heart and pericardium in the middle, and the œsophagus with the vagal nerves below, are anterior to it. The vertebral column is behind. It gives off the bronchial, œsophageal, and intercostal arteries.
The bronchial arteries are two or three in number. They arise from the forepart of the aorta, below the arch. They pass to either side, enter the back part of the root of each lung, and are lost in the cellular tissue of these organs. These arteries sometimes rise from the intercostal, and are very irreoular in number and size.
The œsophageal arteries are also irregular, generally three or four in number. They arise from different parts of the aorta, and send branches to the mediastinum and œsophagus. On the latter, some ascend, some descend. The former inosculate with the cervical arteries, the latter with the abdominal.
The intercostal arteries are usually ten on the left, and nine on the right. They arise from the back part of the aorta, pass obliquely outwards behind the pleura, and enter the intercostal spaces; run along the lower edge of each rib between the layers of muscles, and, about the middle of the chest, divide into an inferior and a superior branch. They both supply the intercostal muscles, and inosculate with the internal mammary and with the thoracic arteries. Each intercostal artery, before entering the intercostal space, sends a large dorsal branch backwards to the muscles on the posterior part of the trunk.
Pl. 135, fig. 9, arch of the aorta, with the thoracic artery: 1, trachea; 2, 3, branch; 4, œsophagus; 5, arch of the aorta; 6, innominata; 7, left common carotid; 8, left subclavian; 9, first intercostal; 10, thoracic aorta; 11, 12, œsophageal arteries; 13, 14, posterior bronchial; 15, an intercostal; 16, its anterior or intercostal branch; 17, its dorsal branch, 18, a branch to the medulla spinalis. Fig. 10, arteries of the spinal marrow, the anterior wall of the vertebral canal removed: 1, spinal marrow inclosed in its sheath; 2, an intercostal artery; 3, a spinal artery entering the intervetebral foramen and ramifying over the spinal marrow and its sheaths.
Abdominal Aorta
The abdominal aorta commences below the tendinous arch, between the crura of the diaphragm in the median line, descends with a slight obliquity to the left, and divides at the lower margin of the fourth lumbar vertebra into the two iliac arteries. The middle sacral may also be considered as one of its terminal branches. It sends off the following branches: the phrenic, cœliac axis, superior mesenteric, inferior mesenteric, renal, supra-renal, spermatic, lumbar, and middle sacral.
1. The Phrenic Arteries arise in common or near each other, from the fore part of the aorta. They both send branches to the supra-renal capsules and to the crura of the diaphragm. The right ascends behind the vena cava, the left behind the œsophagus. On the diaphragm each divides into an external and an internal branch. The former passes towards the circumference of the muscle, and inosculates with the internal mammary and the inferior intercostals; the latter encircles the central tendon.
2. The Cœliac Axis arises from the fore part of the aorta opposite to the last dorsal vertebra; it soon divides into three branches.
a. The gastric artery. This sends branches to the cardiac orifice, to the œsophagus, and to the anterior and posterior surfaces of the stomach.
b. The hepatic artery. This divides ultimately into the right and left hepatic arteries. Previous to this division it gives off the superior pyloric to the upper surfage of the pylorus, and the gastro-duodenalis, which in turn yields infenor pyloric branches, the pancrcatico-duodenalis, and the gastro-epiploica dextra; the first to the lower part of the pylorus, the second to the duodenum and pancreas, and the third to the great omentum and stomach. The right and left hepatic arteries then separate and plunge into the substance of the liver, accompanied by branches of the vena porta; the right hepatic is the larger, and before entering the gland gives off the cystic artery to the gall bladder.
c. The splenic artery. This is the longest branch of the cœliac axis; it passes backwards and to the left side along the upper edge of the pancreas, to which it sends several branches. Near the spleen it gives off the gastro-epiploica sinistra. It next sends off the vasa brevia small branches which go to the great end of the stomach. The splenic artery then divides into several branches, which enter into the spleen.
Pl. 134, fig. 4, the abdominal aorta: 1, diaphragm; 2, kidney; 2′, suprarenal capsule; 3, aorta; 4, 5, 6, visceral arteries cutoff; 7, suparenal artery; 8, renal artery; 9, internal spermatic; 10, a lumbar artery; 11, phrenic artery. Fig. 3, cœliac artery: 1, liver; 2, gall bladder; 3, round ligament of the liver, formerly the umbilical vein; 4, stomach; 5, duodenum; 6, the spleen; 7, pancreas; 8, trunk of the cœliac artery; 9, 11, gastric artery 10, hepatic artery; 12, gastro-epiploica dextra; 13, cystic artery; 14, splenic; 15, outline of the course of the splenic artery behind the stomach; 16, gastro-epiploica sinistra; 17, vasa brevia.
3. Superior Mesenteric Artery. This arises below the cœliac; descends obliquely forwards and to the left behind the pancreas and over the duodenum; it then passes between the layers of the mesentery and takes an arched course towards the right iliac fossa: from its concave side arise three branches, the ileo-colic, the right colic, and the middle colic. These branches proceed between the laminæ of the mesocolon to the large intestine; each dividing into two branches which unite with those on either side and form arches, from whose convexities other subdividing branches again arise and unite as before. These divisions and subsequent inosculations occur several times before reaching the intestine, near which each branch divides into two, which proceed in a direct course, one on the anterior, the other on the posterior surface of the intestine, and are distributed principally to the submucous tissue.
Pl. 134, fig. 45, origin of the superior mesenteric.
Pl. 135, fig. 11, distribution of the superior mesenteric: 1, folds of the small intestines: 2, cœcum; 3, its vermiform appendage; 4, ascending colon; 5, transverse colon; 6, superior mesenteric artery with branches going off to the small intestines, forming numerous inosculations; 7, right colic artery; 8, middle colic.
4. The Inferior Mesenteric Artery arises about two inches below the preceding; it descends towards the left iliac fossa and divides into three branches, the left colic, sigmoid, and superior hæmorrhoidal.
The left colic artery ascends in the left mesocolon, anastomoses with the middle colic branch of the superior mesenteric, and supplies the left part of the colon. The sigynoid artery is distributed to the sigmoid flexure of the colon. The superior hæmorrhoidal descends along the back part of the rectum, supplies the coats of this intestine, and inosculates with the middle and inferior hæmorrhoidal arteries.
5. The Renal Arteries arise from the sides of the aorta, between the superior and inferior mesenteric arteries; both pass behind their corresponding vein and divide near the kidney into five or six branches, which ramify through the substance of this gland.
6. The Capsular Arteries are three in number; they arise either from the renal arteries or from the aorta, and supply the renal capsules.
7. The Spermatic Arteries arise from the fore part of the aorta; in the male they accompany the vas deferens of each side through the spermatic canal, and supply the testis and epididymis; in the female they pass to the ovaries, and also send branches to the Fallopian tubes and to the sides of the uterus.
8. The Lumbar Arteries are four or five pairs. They are analogous to the intercostal arteries, and arise from the back part of the aorta, to be distributed mainly to the muscles of the back and loins.
9. The Middle Sacral Artery arises from the back part of the aorta, a little above its bifurcation; descending nearly in a median line, it sends branches to the sacrum and communicates with the lateral sacral arteries. This is essentially the continuation of the aorta, as may be clearly seen in animals having weak posterior extremities and a highly developed tail.
Pl. 135, fig. 12 1, large intestines; 2, aorta; 3, superior mesenteric; 4, section of one of its branches to the small intestines; 5, right colic artery; 6, a vascular arch of the right colic; 7, boundary between large and small intestines; 8, inferior mesenteric; 9, 10, 11, left colic branch; 12, 13, superior hæmorrhoidal.
Iliac Arteries
The right and left common iliac arteries arise and diverge from the bifarcation of the aorta, which usually occurs on a level with the lower margin of the fourth lumbar vertebra. The point of division, as well as its angle, is, however, variable; nevertheless in the female the angle of bifurcation is always greater than in the male. These vessels descend obliquely outwards as far as the ilio-sacral symphysis, opposite to which, and resting on the psoas magnus, each divides into the external and internal iliac arteries; their length varies from one and a half to two inches.
1. The Internal Iliac or Hypogastric Artery passes downwards in front of the ilio-sacral articulation, describing a curve concave forwards, and reaches the superior part of the sacro-sciatic notch, when it usually divides into a number of branches. From its termination a ligamentous cord (the obliterated umbilical artery of the fœtus) extends to the back and sides of the bladder, and from this to the posterior surface of the recti muscles as far as the umbilicus. It gives off the following branches: ilio-lumbar, lateral sacral, haemorrhoidal, vesical, uterine, and vaginal; the glutseal, sciatic, obturator, and pudic.
1. The ilio-lumbar. This arises from the baek part of the internal iliac and passes into the substance of the iliacus internus, in which it divides into ascending and descending branches. 2. The lateral sacral descends obliquely in front of the sacral lioles, and sends branches to the spinal nerves and to the pyriform muscle. 2. The hæmorrhoidal. These are two or three branches of uncertain origin, which pass to the sides of the rectum and communicate with the superior and inferior hoemorrhoidal arteries. 4. The vesical arteries; these arise from the iliac or some of its branches, and ramify on the coats of the bladder. 5. The uterine and vaginal arteries, arising from the internal iliac or from some of its branches. 6. The glutæal artery passes backwards and outwards from the pelvis by the upper part of the sciatic notch, and divides into several branches, supplying the glutæi. 7. The obturator passes out from the pelvis into the upper part of the thigh, and supplies the obturator and adductor muscles. 8. The sciatic artery escapes from the pelvis through the sciatic notch, and supplies the glutseus maximus, the hamstrings, and the adductor magnus. 9. The internal pudic leaves the pelvis and re-enters it again between the sciatic ligaments; ascending, it divides into two branches a little below the symphysis pubis. On re-entering the pelvis, it gives off: a, the external hæmorrhoidal arteries to the sides of the rectum and anus; b, the perinmal artery to the perinseum and scrotum; c, transversalls perinæi; d, artery of the bulb to the corpus spongiosum urethræ; e, and f, artery of the corpus cavernosum and dorsalis penis.
Pl. 134, fig. 4 12, middle sacral artery; 13, division of the abdominal aorta into the two iliac arteries; 14, division of the iliac arteries into the external and internal iliac arteries; 15, ilio-lumbar; 16, inferior epigastric.
Pl. 135, fig. 13 1, end of the abdominal aorta; 2, middle sacral; 3, a lumbar artery; 4, common iliac artery; 5, femoral or external iliac artery; 6, circumflex ilii; 7, inferior epigastric; 8, umbilical artery; 9, obturator; 10, vesical; 11, ilio-lumbar; 12, 13, lateral sacral; 14, superior glutæal. Fig. 14, obturator artery, and its division into an anterior and a posterior branch in the upper part of the thigh.
2. The External Iliac Aetery proceeds from the common iliac, downwards and outwards to Poupart’s ligament, beneath which it passes, and then receives the name of femoral. Near the groin it gives off two branches: 1. Circumflex ilii, which, arising from its outer side, ascends obliquely outwards as far as the crest of the ilium, where it branches to go to the abdominal muscles, and to the iliacus internus and quadratus lumborum; 2. The epigastric artery, which arises from the fore part, a little above Poupart’s ligament, and, first descending, ascends between the abdominal muscles and the peritonœum, ultimately reaching the rectus muscle, the umbilicus, and the internal mammary artery.
3. The Femoral Artery, the continuation of the external iliac, descends from the middle of the crural arch, along the anterior and internal part of the thigh. It sends off—
a. Some superficial branches, as the inguinal, to the inguinal glands; the superficial pubic, to the pubes; the superficial epigastric; and the external circumfiex ilii, to the skin about the crest of the ilium.
b. The profunda. This, the largest branch of the femoral, arises about two inches below the crural arch, from the outer and back part of the femoral artery, and descends behind it. At the back part of the thigh it terminates in two branches for the hamstring muscles, and in its course gives off the two circumflex, and the three perforating arteries. The external circumflex arises from the outer part of the profunda, and, passing transversely beneath the sartorius and rectus muscles, divides into three fasciculi of branches. The internal circumflex arises near the preceding, sometimes from the femoral itself, and passes to the back part of the thigh. The first, or superior perforating artery, passes backwards beneath the lesser trochanter to the adductor magnus and to the hamstring muscles. The second, or middle perforating artery, passes through the adductor magnus and brevis to the muscles on the back of the thigh. The third, or inferior perforating artery, descends behind the adductor longus to the hamstrings. On the back part of the thigh the profunda ends in two branches, of which one passes to the biceps, the other to the semi-membranosus.
c. After the origin of the profunda, the femoral gives off several small twigs, and near the opening in the triceps it gives off a third, the anastomotica magna, which descends in front of the adductor tendon to the knee, and sends several branches to the integuments, vastus externus, and to the patella.
4. The Popliteal Artery descends from the inner side of the femur, outwards to the inferior and central part of the poplitseal space. Its branches are: 1. Several muscular branches to the hamstrings, and to the gastrocnemius; 2. Superior articular, which encircle the lower extremity of the femur, and communicate with the anastomotica; 3. Azygos articular, passing forwards through the posterior ligament of the joint to the synovial membrane, and the adipose substance in its cavity; 4. Inferior articular arteries, which encircle the lower part of the joint to its fore part, and inosculate with the preceding, and with the anterior tibial recurrent. At the lower part of the ham the poplitasal divides into the anterior and posterior tibial arteries.
5. The Anterior Tibial Artery perforates the interosseous space close to the head of the fibula, descends along the interosseous membrane, and over the lower part of the tibia, to the first interosseous space. It gives off: 1. The recurrent to the articulation of the knee; 2. Muscular branches to the muscles on the outer and anterior part of the leg; 3. Malleolar branches to the internal and external malleoli; 4 and 5. Tarsal and metatarsal; between the two first metatarsal bones it divides into, 6, the anterior pollicis to the integuments, and 7, communicans to the first interosseal muscles.
6. The Posterior Tibial Artery descends between the superficial and deep layer of muscles on the back of the leg, to the space between the heel and inner ankle, where it divides into the external and internal plantar arteries. It gives off: 1. Several muscular branches; 2. The peronæal artery. This arises about an inch below the poplitæal, and, descending to the ankle, divides into the anterior and posterior peronæal branches. The former pierces the interosseous ligament, and inosculates with the external malleolar; the latter spreads its branches on the outer side of the heel and of the foot.
The internal plantar artery proceeds along the internal side of the sole, and inosculates with the adjacent vessels. The external plantar, much the larger, passes forward as far as the fifth metatarsal bone; it then crosses the metatarsus, and joins the anterior tibial, to form the plantar arch.
Pl. 135, fig. 15 1, sartorius muscle, cut off; 2, hole in the tendon of the adductor magnus; 3, femoral artery; 4, superficial epigastric; 5, profunda artery; 5′, 5′, perforating branches of the profunda; 6, internal, 7, 8, external circumflex arteries; 9, 10, superficial pudic; 11, poplitaeal artery. Fig. 17 1, anastomotica; 2, anterior tibial; 3, recurrent branch; 4, external, 5, internal malleolar; 6, tarsal vessels; 7, metatarsal vessels; 8, an artery of the toes. Fig. 16, plantar arteries: 1, posterior tibial artery; 2, internal, 3, external plantar arteries; 4, deep plantar arch; 5, a branch to the back of the foot. 6, a metatarsal artery; 7, its division into two branches; 8, union of two such branches; 9, division into the arteries of the toes; 10, union of two such divisions; 11, vascular plexus at the tip of the toes.
The Veins



The veins commence in the capillary system, and are therefore continuous with the arteries: in some parts they appear to arise out of a cellular or spongy intermediate structure, although this may be nothing more than a venous plexus. From the origins the veins unite and form larger branches, which ultimately end in two great trunks. Both small and large veins are remarkable for their numerous anastomoses, and large veins are often seen to divide and unite again.
Veins are composed of the same number of coats as arteries, but the middle lamina is much thinner, therefore they collapse when empty or when divided. The external or cellular coat is similar to that of arteries; the middle or fibrous coat wants the external elastic lamina, but possesses the two other layers of contractile fibres, the external circular and the internal longitudinal; the third, or innermost, or serous coat is stronger, but similar to that of the arteries, being, indeed, continuous with it through the capillaries on the one hand, and the cavities of the heart on the other. The most striking peculiarity in this tissue is seen in the presence of numerous semi-lunar folds or valves; each of these is composed of a duplicature of the membrane, inclosing some fibrous cord. Their concave floating end is towards the heart, and therefore the blood in its course towards this organ meets no resistance from the valves, while they present serious obstacles to its reflux. These valves are sometimes in pairs, sometimes single; they are most numerous in the extremities and in the deep veins, and are generally found at points of confluence; they are absent in very small veins, and in the large trunks, as the cavae, iliacs, internal jugular, and innominata; also in the cerebral veins, and in the whole of the portal system.
In the descriptive anatomy of the veins, we divide the whole into the deep and the superficial; the former are called “venæ comites,” as they generally accompany the arteries. As the latter of course have much the same distribution as the arteries, the superficial veins will alone require especial attention.
All the venous blood of the body empties into the heart through the two venæ cavæ, excepting that of the heart itself, which is poured directly into the right auricle by the coronary or cardiac vein. We shall begin with the description of the branches of the superior vena cava, belonging to the head, neck, thorax, and superior extremities, although, owing to the great number of the veins and their incessant anastomoses, it will be impossible to classify them with the precision of which the arteries are generally capable.
Veins of the Head and Neck
The veins of the head and neck are superficial and deep: the superficial veins of the head return the blood from the scalp; the deep veins are those of the brain and sinuses.
It may on the whole be said that the superficial veins return the blood circulated by the external carotid artery, while the deep veins bring back that of the internal carotid. Starting at the heart, we find the superior vena cava subdivided into two large veins, the right and left venæ innominatæ or brachio-cephalic veins. Each of these is formed by the union of the subclavian and internal jugular of each side, the subclavian subdividing into the external jugular and axillary veins. The superficial veins of the head converge and unite so as to form two trunks, the facial and the temporal; the former empties into the internal jugular vein, the latter into the external.
The Facial Vein lies obliquely along the sides of the face, extending from the inner margin of the orbit downwards and backwards to the anterior edge of the masseter muscle. Resting on the same plane with the facial artery, it maintains nearly the same relations. It commences at the side of the root of the nose by a vein formed by the conflux of branches from the forehead, eyebrow, and nose, and increases by receiving others at each step of its course.
The frontal vein commences on the roof of the skull by branches which pass obliquely downwards and forwards on the forehead, maintaining communication with the anterior branches of the temporal. By the successive union of different branches, a vein of some size is ultimately formed, which descends vertically, parallel with the corresponding vessel of the opposite side, with which it is connected by transverse branches. When descending from the forehead, it receives branches from the eyebrow, the nose, and the upper eyelid.
The supra-orbital vein runs transversely inwards in the direction of the eyebrow; its radicles are coDnected externally with those of the external palpebral and superficial temporal; in its course it receives branches from the contiguous muscles and integuments, and at the inner angle of the orbit it inclines downwards to form the frontal vein. The two by their junction form the angular vein, which runs downwards and outwards by the inner margin of the orbit, resting against the side of the root of the nose. It receives the vasal veins from the side and ridge of the nose and some small palpebral veins open into it from the opposite direction. When arrived on a level with the lower margin of the orbit, the angular vein terminates by becoming continuous with the facial vein.
The facial vein, thus started, increases by recurving branches from the lower eyelid, and from the ala of the nose and from its outer side, the inferior palpebral vein. Lower down it is joined by branches from the lip and cheeks, and uniting with a branch from the temporal vein, empties into the trunk of the internal jugular. Previously, however, it receives the ranine vein, from the tongue, the submental vein, and the palatine vein.
The Temporal Vein is a vessel of considerable size, extending from the zygoma to the angle of the jaw, while its branches spread out on the sides of the head. The principal of these branches are, the posterior temporal, the middle temporal, and the anterior temporal. Sinking below the angle of the jaw, it divides into two branches, of which one joins the facial vein, and the other becomes continuous with the external jugular vein. Other branches opening into the temporal vein are, the parotid, the articular, the auricular, the transversalis faciei, and the auricularis posterior. A vein of considerable size, joining the temporal in the parotid gland, is:
The internal maxillary. This receives branches from the temporal fossa, from the pterygoid muscles, from the surface of the upper jaw, and from the lower through the dental foramen.
The External Jugular Vein commences on a. level with the angle of the jaw by the union of two branches, one the communicating branch from the termination of the temporal vein, the other from the mastoid region. Descending vertically, it unites with the subclavian. The principal veins which open into it are, the anterior jugular from the fore part of the chin, and from the scapular region, the supra-scapular and the posterior scapular.
Cerebral Veins. The venous system within the skull consists of veins properly so called, and sinuses or reservoirs. The former we shall not consider in this place. The sinuses of the cranial cavity may be divided into two sets, those placed in the prominent folds of the dura mater and those disposed at the base of the skull. The former all converge more or less to a common point, which corresponds to the internal occipital protuberance, and is called the torcular herophili. The sinuses are as follows: 1. The superior longitudinal sinus, extending from before, backwards in the upper part of the falx cerebri, and commencing at the crista galli. 2. The inferior longitudinal sinus. This very small sinus is placed in the inferior concave border of the falx, and opens into the straight sinus. 3. The straight sinus, a continuation in a measure of the last, runs backwards in the direction of the base of the falx cerebri. 4. The lateral sinuses. Their direction conforms to that of the groove on the interior of the occipital bone, and passing from the protuberance to the foramen lacerum posterius. 5. The postenor occipital sinus, which conducts from the posterior margin of the foramen magnum to the torcular.
The basal sinuses are, the circular, the cavernous, the superior petrosal, the inferior petrosal, and the occipital.
The Internal Jugular Veins. The blood from the brain and cranial cavity is received by the internal jugular veins, which are continuous at their upper extremities with the lateral sinuses and terminate inferiorly in the venæ innominatæ. The junction of the internal jugular vein with the lateral sinus takes place in the broad part of the foramen lacerum. Passing down to a level with the os hyoides, it receives the common trunk of the facial and temporal veins, and then enlarges considerably. Previously to the junction with the facial vein, it receives the lingual vein from the tongue, the pharyngeal from the back and sides of the pharynx, the superior thyroid and the occipital from the back of the head.
The Vertebral Veins commence among the deep muscles beneath the occiput, inosculate with the occipital vein, and enter the canal in the transverse processes between the foramen magnum and the atlas. Descending they receive various muscular branches, and empty into the subclavian vein nearly opposite to and behind the internal jugular.
Inferior Thyroid or Tracheal Veins form a plexus in front of the trachea. They commence about the thyroid body, and open into the vena innominata or into the cava.
The Venæ Innominatæ. These, as already remarked, unite to form the superior vena cava. The left vena innominata is about three inches long, and receiving the thoracic duct at its commencement, is joined in its course by the left vertebral, the inferior thyroid, internal mammary, superior phrenic, and mediastinal veins. The right vena is an inch in length, and descends almost perpendicularly. It receives at its commencement the right absorbent trunk, and in its course the right vertebral vein, and sometimes the right inferior thyroid and right mammary and mediastinal veins.
The Superior Vena Cava descends from the confluence of the venæ innominatæ almost vertically, enters the pericardium, and opens into the right auricle behind its appendix. The vena azygos joins it just before it enters the pericardium. It returns the blood from the supra-diaphragmatic part of the body, and communicates with the inferior vena cava through the vena azygos and the vertebral veins.
The Azygos Veins constitute important appendages to the venæ cavæ, maintaining numerous communications between their branches, securing the course of the circulation, notwithstanding any local impediment in any particular vessel. The right or greater azygos commences in the abdomen, and ascending through the aortic passage of the diaphragm, empties into the back part of the superior cava. It receives several branches, and drains the thorax.
Pl. 133, fig. 1, superficial veins of the head and neck: 1, pericardium displayed; 2, right auricle; 3, superior vena cava invested by the pericardium; 4, do. above the pericardium; 5, right subclavian; 6, root of the internal mammary vein; 7, left subsclavian vein; 8, internal jugular; 9, thyroid; 10, transverse cervical and scapular veins; 11, anterior facial vein; 12, its union with the ophthalmic vein; 13, frontal vein; 14, occipital vein; 15, superficial temporal vein; 16, axillary vein; 17, the cephalic vein.
Pl. 136, fig. 1 1, right auricle; 2, superior vena cava; 3, internal mammary; 4, a vein of the diaphragm; 5, right subclavian vein; 6, right internal jugular vein; 7, right external jugular; 8, left subclavian; 9, lower thyroid; 10, left mammary; 11, left internal jugular; 12, left external jugular. Fig. 7, sinuses of the falx cerebri: 1, superior longitudinal sinus; 2, inferior do.; 3, straight sinus; 4, great meningeal vein; 5, confluence of the sinuses. Fig. 8, sinuses at the base of the skull: 1, place of entrance of the superior longitudinal sinus into the torcular; 2, horizontal portion of the lateral sinus; 3, its descending portion; 4, mouth of the internal jugular; 5, superior petrosal sinus; 6, cavernous sinus; 7, transverse branch along the sella turcica to form the transverse sinus. Fig. 9, point of confluence of the sinuses or the torcular herophili, opened: 1, superior longitudinal sinus; 2, opening of the straight sinus; 3, 3, openings of the posterior occipital sinuses; 4, 4, openings of the lateral sinuses. Fig. 10, a parietal bone, with the outer table removed to show the diploic veins.
Veins of the Superior Extremities
The veins of the upper extremities are superficial and deep. The principal superficial veins are the cephalic, basilic, and median. The superficial veins of the hand are principally on the dorsal aspect. On the back of the hand there is a venous arch or series of arches, which receive two freely anastomosing veins from each finger. From this arch branches ascend, two of which being larger and more regular, have received distinct names, cephalic and basilic.
The cephalic vein commences on the outer and back part of the carpus, ascends to the bend of the elbow, and continuing along the outer side of the biceps, turns forward towards the shoulder, and sinks deep between the pectoral and deltoid muscles to join the axillary vein.
The basilic vein commences from the dorsal arch near the lower end of the ulna. One branch from the little finger is termed salvatella. Ascending along the ulnar side of the forearm, it passes before the internal condyle, and continuing up the inner side of the arm, joins the axillary vein.
The median vein arises a little above the wrist, and ascends along the middle of the forearm to the bend of the elbow. It here divides into two branches; one (median basilic) joins the basilic vein, the other (median cephalic) joins the cephalic vein.
The deep veins accompanying the brachial artery and its branches in the arm and forearm, two with each inclosed in the same sheath. These end in the
Axillary Vein, which ascends in front of the artery, receives the thoracic veins, passes beneath the clavicle, and opposite the lower edge of the first rib is named
Subclavian Vein. This passes inwards, receiving several veins from the shoulder and sides of the neck, as also the jugular veins, and opposite the sterno-clavicular articulation, unites with the internal jugular, as already described, to form the vena innominata.
Pl. 133, figs. 2 a, b, superficial veins of the arm on the inside; fig. 2 a 1, axillary vein; 2, 3, cephalic vein; 4, median vein passing into the cephalic; 5, basilic vein; 6, its dorsal branch; 7, anterior branch; 8, median vein passing into the basilic; 9, common trunk of the median vein. Fig. 3, plexus on the back of the hand and forearm: 1, cephalic vein; 2, its origin at the thumb; 3, basilic vein; 4, its origin at the little finger. Fig. 4, veins at the bend of the elbow, used in blood-letting: 1, opening in the brachial aponeurosis, showing the course of the brachial artery and vein, with the relative position of the median nerve; 2, cephalic vein; 3, a branch; 4, median vein passing into the cephalic; 5, basilic vein; 6, dorsal branch; 7, anterior branch; 8, 9, stem of the median vein.
Pl. 136, fig. 1 13, stem of the intercostal veins of the left side; 14, 15, union of such veins; 16, hemiazygos vein; 17, inferior cava. Fig. 2, azygos and hemiazygos (lesser azygos) veins: 1, superior vena cava; 2, azygos vein; 3, upper intercostal vein of the left side; 4, 5, venous trunks uniting to form the hemiazygos; 6, branches uniting to form the azygos; 7, inferior cava; 8, 9, 10, intercostal veins uniting partly with the azygos, partly with the superior intercostals, and partly with the hemiazygos. Fig. 5, venous plexus on the anterior wall of the vertebral canal: 1, two longitudinal trunks; 2, transverse connecting branches; 3, branches passing through the intervertebral foramina, and communicating with the external plexus. Fig. 6, plexus on the posterior wall of the vertebral canal: 1, the two longitudinal trunks; 2, the transverse connecting branches; 3, intercostal veins uniting with the inner plexus.
Veins of the Inferior Extremities
The veins of the lower extremities are superficial and deep. The general course of these veins (commencing at the feet) is as follows: the superficial veins of the foot feed the external and internal saphena veins, which empty, the former into the poplitaeal vein, the latter into the femoral, which is itself only a continuation of the poplitæal. The femoral, after it is joined by the profunda and saphena veins, becomes the external iliac, which unites with the internal iliac, to form the common iliac. Finally the common iliacs of the two sides unite to form the inferior or ascending vena cava.
The External Saphena Vein passes from the dorsum of the foot behind the external malleolus, and joins the poplitæal.
The Internal Saphena commences at the upper and inner part of the foot, and ascends in front of the inner ankle, along the inner side of the leg, and behind the internal condyle of the knee. Inclining to the internal and anterior part of the thigh, it ascends to within about two inches of Poupart’s ligament, passing through the saphenic opening of the fascia lata to join the femoral vein. It receives numerous branches throughout its course.
The deep veins of the leg, accompanying the arteries, two with each, and terminating in the following:
Poplitæal Vein. This lies posterior to the artery, and receives the posterior saphena vein, with numerous branches: ascending obliquely inwards, it passes through the opening in the tendon of the triceps to become the
Femoral Vein, which is joined in the groin by the profunda and saphena veins to form the
External Iliac Vein. This extends from Poupart’s ligament to the ilio-sacral symphysis, where it meets the internal ihac to form the common iliac. It also receives the trunk of the epigastric veins, and of the two circumflex ilii.
The Internal Iliac Vein accompanies the artery in its inner side; it is formed by the union of several veins corresponding to the branches of the internal iliac artery, viz. obturator, pudic, sciatic, glutceal, &c.
The Common Iliac Veins are formed by the union of the two internal and external, opposite each ilio-sacral symphysis. Ascending, they meet at an acute angle, opposite the fourth intervertebral ligament to the right side of and little below the division of the aorta. Their union constitutes the inferior or ascending vena cava.
The Inferior Vena Cava, thus constituted, ascends along the right side of the aorta, passes through the diaphragm, and opens into the lower and back part of the right auricle. It receives the lumbar, spermatic, renal or emidgent, capsular or supra-renal, inferior phrenic, and the hepatic veins. The inferior cava is larger than the superior; it returns the blood from all parts of the body below the diaphragm, collecting that of the portal system through the medium of the hepatic veins.
Pl. 136, fig. 1 18, hepatic vein; 19, internal spermatic; 20, supra-renal; 21, renal veins; 22, connecting branch between the renal and common iliac veins; 23, 24, lumbar veins; 25, common iliac; 26, femoral; 27, hypogastric; 28, 29, 30, lateral and middle sacral veins.
Pl. 134, fig. 7 1, internal saphena vein; 2, exterior epigastric; 3, an accessory, and 4, a principal branch of the internal saphena. Fig. 8 1, course of the internal saphena on the inside of the leg; 2, its commencement on the back of the foot. Fig. 9, plexus on the back of the foot. Fig. 10 1, external saphena; 2, internal do.
The Portal System
The portal system constitutes a peculiar vascular arrangement in the liver for the purification of the blood and the secretion of the bile. The portal vein, or vena porta, although it arises in the abdomen as a vein, and serves the same office, yet terminates in the liver like an artery, and has a secreting function; it returns the blood from all the chylopoietic viscera, to be distributed through the liver, and in the latter organ it receives the venous blood from the termination of the hepatic artery. It is four or five inches long, and is formed by the confluence of the splenic and mesenteric veins behind the pancreas. Ascending obliquely, it receives branches from the pancreas, duodenum, stomach, and gall-bladder, and enters the left extremity of the left fissure of the liver, there to divide into right and left branches, which in the liver become subdivided into smaller branches divisible into three orders: vaginal, interlobular, and lobular. The lobular branches constitute the ultimate ramifications, entering and forming a plexus in each lobule of the liver; they are then continued into the intralobular veins, which unite in the sublobular, these combining to form the hepatic trunks of the hepatic veins which pour their blood into the inferior vena cava. In the lobules, the venous blood is depurated by the secretion of the bile, which pours into the hepatic ducts. The object of the hepatic artery is probably nutritive, and not secreting as formerly supposed.
Pl. 133, fig. 5 1 liver; 2, gall-bladder and duct; 3, hepatic artery; 4, inferior vena cava; 4′,4′, head of the pancreas; 5, 5, the two posterior sections of the duodenum; 6, 6, 6, 6, folds of the small intestines; 7,cœcum and ascending colon; 8, descending colon and rectum; 9, spleen; 10, stomach turned back; 11, 11, veins of the jejunum and ileum; 12, right vein of the ileum; 13, superior mesenteric vein; 14, 14, splenic vein; 15, lesser mesenteric vein; 16, left plexal vein of the stomach; 17, left coronary vein of the stomach; 18, 19, trunk of the vena porta; 20, umbilical vein.
The Lymphatics
Absorption, so necessary to nutrition, is effected by means of minute vessels termed absorbents, and the small reddish bodies termed absorbent or conglobate lymphatic glands, through which the absorbents pass. The absorbents are divided into two classes, named lymphatics and lacteals. The lacteals are found only in the abdomen, and are so called from the milky appearance of the chyle which they absorb from the intestinal villi, and which is conveyed by their trunk, the thoracic duct, into the general circulation. The lymphatics are so named from the clear fluid or lymph they contain; they are distributed through all parts of the body, and their office is to absorb in every tissue all matters that have become effete or useless: these, being first reduced to a state of solution, are conveyed into the general circulation, either to be discharged from the system by some of the excretory organs, or to undergo certain changes fitting them again for the purposes of the animal economy. The lymphatics are arranged, like veins, into superficial and deep; the former accompany the subcutaneous veins, the latter the deep-seated vessels; they run very much parallel to each other, often bifurcate, and either soon reunite or join similar adjacent branches: as they approach any of the glands they converge, each divides into two, which inclose its extremity, and soon enter through its surfaces; these are the vasa inferentia. Within the gland they subdivide and inosculate so as to form an inextricable plexus; from this, branches again issue and leave the gland by the opposite end; these are the vasa efferentia, and are larger, but fewer, than the vasa inferentia. All absorbents pass through one gland at least, and some through more, before they empty into the venæ innominatæ. The structure of the absorbents is very similar to but more delicate than that of veins; they have three coats, but the middle, as in the veins, is thin, and wants the elastic lamina.
The lymphatic or conglobate glands are very numerous both in the extremities and in the trunk; their size varies from that of a small currant to that of an almond; the largest are in the groins and in the roots of the lungs. Their form is round, or irregular and lobulated.
The Lymphatic Vessels of the Lower Extremities. These are superficial and deep. The superficial commence from the toes, rise along the dorsum of the foot, and pass up the leg in two divisions, which, however, frequently communicate: one, the internal group, passes in front of the inner ankle, and keeps parallel and close to the great saphena vein; these branches ascend to the groin, and pass through the inferior superficial gland into the external iliac gland. The external set of superficial lymphatics ascend behind the inner ankle, accompany the external saphena vein to the ham, pass through the glands there situated, and join the deep lymphatics of the limb.
The lymphatics of the trunk and viscera are very numerous and exceedingly complicated. The absorbents of the small intestines are either lymphatics or lacteals; the former arise in the subserous tissue, the latter in the submucous tissue and in the villi. The lacteals proceed at once from the intestine into the mesentery and its glands: they take up the chyle and pour it into the thoracic duct.
The thoracic duct, great or left, is the common recipient of the absorbents not only of the infra-diaphragma.tic portion of the body, but also of those of the left side of the chest, head, neck, and left arm. It commences by the confluence of a variable number of branches, in a common reservoir or dilatation called receptaculum chyli, which is placed to the right and somewhat behind the aorta, and rising into the neck, arches forwards and downwards, opposite the seventh cervical vertebra, and empties into the angle between the left subclavian and jugular veins, protected by a pair of valves against regurgitation from these vessels.
The head, face, and neck are well supplied with lymphatics. Ten, however, occur in the cranium, and none have as yet been detected in the brain. In the upper extremity, the superficial lymphatics commence from the fingers and the back part of the hand, and accompany the subcutaneous veins. The deep lymphatics follow the individual blood-vessels, reach the axillary glands, and receive various branches. On the left side they accompany the subclavian vein and join the descending portion of the thoracic duct. On the right side, the axillary or subclavian lymphatics, joined by the right cervical, form a short trunk about an inch in length, termed the right lymphatic duct. This trunk opens into the angle between the right subclavian and jugular veins; it is the termination of the lymphatics of the right arm, right side of the thorax, and of the head and neck.
Pl. 136, fig. 14 1, superior vena cava; 2, azygos vein; 3, thoracic duct; 4, portion of the pelvic plexus; 5, external iliac do.; 6, lumbar do.; 7, receptaculum; 8, point of union of the chyliferous vessels of the intestinal canal, with the thoracic duct; 9, 9, intercostal lymphatics; 10, 10, deep lymphatics of the lungs; 11, entrance of the thoracic duct into the subclavian vein; 12, right lymphatic duct.
Pl. 133, fig. 13 1, common carotid artery; 2, internal jugular; 3, external do.; 4, axillary artery; 5, axillary vein; 6, a lymphatic vessel on the anterior of the breast; 7, 7, axillary plexus; 8, 8, 8, superficial lymphatics of the cranium; 9, 9, superficial lymphatics of the face; 10, anterior glands of the ear; 11, sub-maxillary gland; 12, 12, lymphatic vessels and glands of the neck.
Pl. 136, fig. 15 1, median vein; 2, 2, superficial lymphatics of the arm; 3, axillary glands. Fig. 16, deep lymphatics: 1, 1, 1, deep veins of the forearm; 2, 2, 2, lymphatics accompanying them; 3, lymphatic glands in the bend of the arm; 4, 4, 4, veins of the arm; 5, 5, their accompanying lymphatics; 6, a gland of the arm; 7, axillary gland.
Pl. 133, fig. 12 1, lymphatics of the lower part of the trachea; 2, heart with its superficial lymphatics; 3, 3, superficial lymphatics of the lungs. Fig. 6, superficial lymphatics of the foot. Fig. 7, superficial lymphatics of the inferior extremity: 1, lymphatics accompanying the great saphena vein; 2, superficial inguinal glands; 3, superficial lymphatics of the lower part of the abdomen and loins. Fig. 8, superficial posterior lymphatics of the lower part of the leg. Fig. 10, deep lymphatics of the anterior part of the leg: 1, anterior tibial vein; 2, 2, its accompanying lymphatics; 3, anterior tibial glands; 4, superficial lymphatics of the lower part of the thigh. Fig. 11 a b, anterior deep lymphatics of the thigh and pelvis: 1, femoral vein; 2, deep femoral vein; 3, external iliac vein; 4, lumbar vein; 6, 6, deep lymphaticsof the thigh; 7, deep inguinal glands; 8, femoral plexus; 9, iliac plexus; 5, 10, lumbar plexus.
Pl. 134, fig. 11, deep lymphatics of the posterior face of the thigh: 1, 1, lymphatic glands of the ham; 2, 2, deep lymphatics of the thigh; 3, iliac plexus; 4, lymphatic vessels between the glutæi muscles. Fig. 12, deep lymphatics of the posterior part of the leg: 1, posterior tibial vein; 2, peronaeal vein; 3, poplitaeal vein; 4, 4, lymphatics of the tibia; 5, of the fibula; 6, 6, 6, lymphatic vessels and glands of the ham.
![]() The Nervous System (Neurology)
The Nervous System (Neurology)
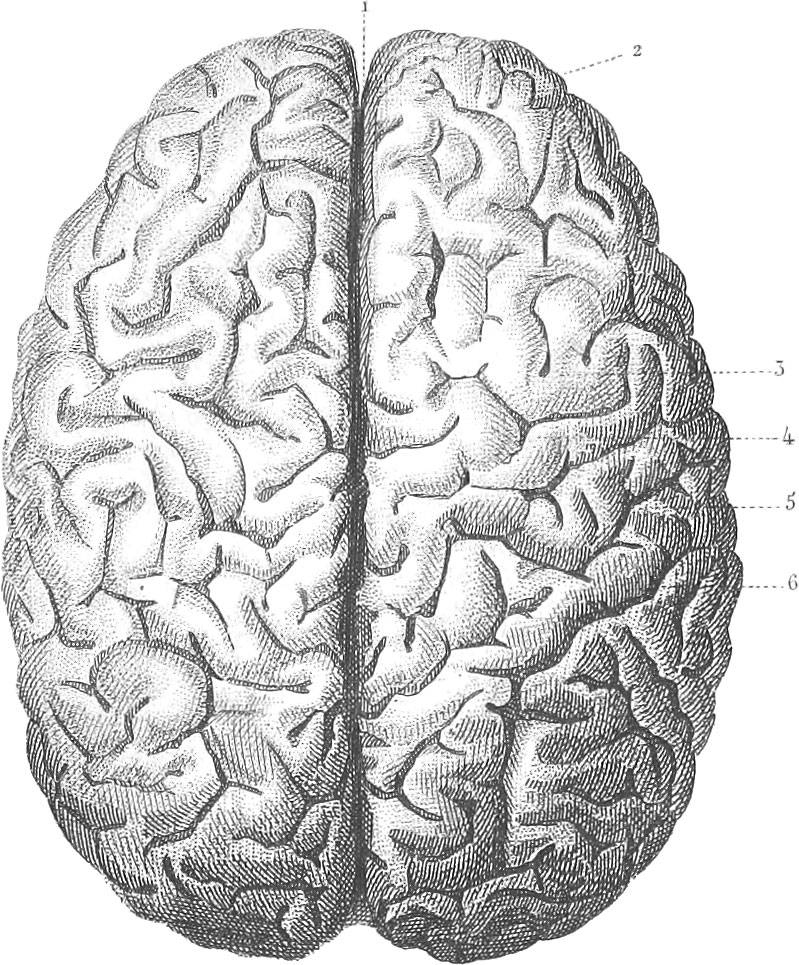 The Nervous System (Neurology)
The Nervous System (Neurology)General Considerations
The nervous system, like the vascular, is distributed throughout all parts of the body, all the vital operations being subjected to its influence. It consists of two systems differing essentially in many respects, yet closely connected in many places: one, the animal, constituting the principal medium of communication between the organism and the external world by means of sensation, motion, and perception; the other, the vegetative or sympathetic, devoted essentially to the functions of assimilation and nutrition. The two are closely related to each other, and the influence of the former on the latter is not to be mistaken.
Each nervous system has a central and a peripherical portion. The central portion of the animal system is the brain and spinal marrow, the peripherical the white thread-like nerves which proceed from these to the various organs and back again. In the sympathetic system, the central portion is constituted by two cords, one on each side of the median line of the body, with ganglia or knots placed at intervals all along.
There are two kinds of structure visible in the nervous system, the white or fibrous and the grey or cineritious. The white matter with the neurilema or nerve sheath and the areolar tissue which it incloses, constitutes the whole of the nervous trunks, wherever they occur, and forms a large part of the central masses with which they are connected. It consists of tubes of great minuteness, which are composed of an interlacement of extremely delicate fibres. When examined immediately after death, the contents of these tubes appear pellucid and homogeneous, and of a fluid consistence; subsequently, however, this contained substance coagulates, and is seen distinct from its investment. The diameter of the cylindrical nervous tubuli varies from 1-2000th to 1-6000th of an inch; the fibres decrease, however, as they approach the brain. The nerve matter in the tubes originally consists of nucleated cells.
The other elementary form of nervous structure is the cineritious or reddish grey matter. It appears to consist principally of a plexus of blood-vessels into which the fibres of the first form may be traced, and amongst these lie a number of nucleated globules without any very definite arrangement. This substance is usually disposed in the interior of the larger masses with which the nervous trunks are connected. It occupies part of the interior of the spinal cord and of the ganglia, but in the brain it is disposed externally, forming a coating to the subjacent mass, which consists almost entirely of fibrous structure; hence it is called sometimes the cortical substance, as distinguished from the medullary, or the fibrous portion. The ganglion globules are from 1-300th to 1-1250th of an inch in diameter, possessing a spherical or oval form, more or less flattened, and having a reddish color. Each contains one or more nuclei with subordinate nucleoli, and is inclosed in a very fine filamentous investment, in which it is commonly found to be loosely suspended. The sheaths of the several globules are connected with each other by prolonged filaments or peduncles, and these form a kind of network, which occupies the interstices of the fine vascular plexus by which every part of the grey matter is traversed.
If we examine one of the cerebro-spinal nerves, we shall find it to be invested by a sheath of membrane already referred to under the name of neurilema. Its office is chiefly mechanical, namely, that of binding together the constituent fibrillæ and fascicles of the nerve, so as to protect them, and support the delicate plexus of capillary blood-vessels from which they derive their nutriment. To the naked eye the neurilema exhibits the appearance of a white and almost silvery membrane.
After the external part of the neurilema has been removed, the nerve may be divided into secondary bundles composed of the ultimate or primitive fibres. The composition of these has been already referred to. They present the appearance of a series of transparent tubes placed in simple juxtaposition without any intercommunication.
The main trunk of a nerve breaks up into its component bundles, as it passes from centre to periphery, yielding up branches to the various parts it is destined to connect with the nervous centre. These branches generally come off at acute angles, and soon plunge into the muscles and other parts to which they tend, dividing and subdividing as they proceed. An exception to this mode of branching is where a branch separates from the parent trunk at an acute angle, and then turns to run in an opposite direction, forming an arch, from the convexity of which several branches are given off; such a nerve is said to be recurrent.
In their branchings, nerves subdivide, not only to pass immediately to their muscles or other distant parts, but also to connect themselves by certain of these filaments with other nerves, and to follow the course of the latter, instead of adhering completely to that of the parent trunk. By these means nervous filaments, connected with very different parts of the brain and spinal cord, become bound together in the same fasciculus, and a nerve is formed, compounded of tubes possessing very opposite functions. The anastomosis of nerves formed in this manner differs essentially from the anastomosis of blood-vessels, in there being not the slightest communication of the contents of the nervous tubes, as there is in the vascular.
The plexuses are nervous anastomoses of the most complicated and extensive kind. Those which are connected with the spinal nerves are found in the neck, the axillas, the loins, and the sacral regions. There are also plexuses connected with the fifth nerve, the portio dura of the seventh, the glosso-pharyngeal, and the par vagum. Each plexus is formed by the breaking up of a certain number of nervous trunks, the subdivisions of which unite to form secondary nerves, and these again, by further interchange of fibres, give rise to nerves which emerge from the plexus, and consequently in their construction may derive their fibres from several of the trunks that enter the plexus.
The object of the anastomosis of nerves appears to be to associate together nervous fibres connected with different parts of the brain or spinal cord. In this manner, nerve-tubes of different properties or endowments become united together in one sheath, forming compound nerves; and certain sets of muscles, instead of receiving their nerves from a very limited portion of the cerebro-spinal centre, are supplied from a considerable extent of that centre, and each muscle may probably receive nerves which arise in different and distant parts of the spinal cord or brain; an arrangement whereby remote parts of those centres may be brought into connexion with neighboring muscles or other parts, or even with a single muscle.
The nerves serve to conduct impressions from the external world to the nervous centres, or to transmit volitions from these centres to the structure at large, and especially to the muscular system. The former are called afferent or sensory nerves, the latter efferent or motor, and the two are usually bound up together ia the same sheath. The precise relations of these two sets of fibrous nerves to each other and to the nervous centres will be subsequently referred to.
We shall now proceed to consider the special anatomy of the nervous system, under the heads of the brain, the spinal cord, the nerves, and the ganglions.
Anatomy of the Brain

Membranes of the Brain and Spinal Cord
The brain is that ganglionic enlargement of the cerebro-spinal axis seen at its anterior extremity, and characterizing the nervous system of the vertebrata, as distinguished from the invertebrata. Deferring for the present any further account of its intimate structure, we find it to be invested with three membranes or meninges: one, fibrous and external, the dura mater; one, serous and median, the arachnoid; and a third, vascular and internal, the pia mater.
1. Dura Mater. The dura mater is a dense membrane, composed almost entirely of white fibrous tissue. It has all the characters, physical and vital, of that texture, possessing great strength and flexibility, with but little elasticity. It is freely supplied with blood-vessels, and at certain situations it separates into two laminse, which inclose prolongations of the lining membrane of the venous system, forming peculiar sanguiferous channels, known as sinuses (see p. 97). It has an apparently laminated appearance, from the fact of its fibres being disposed in different planes; indeed, in the child a subdivision into two layers may sometimes be easily effected. Some nerves have been demonstrated in the dura mater.
The spinal dura mater is in shape adapted to the vertebral canal, consisting of a hollow cylinder, tapering somewhat at its lower extremity to correspond with the sacral portion of the canal. It adheres very firmly around the foramen magnum, from which it is continued downwards to the sacrum, without forming any adhesion to bone.
On the sides the dura mater is perforated by orifices, which give exit to the roots of the nerves which arise from the spinal cord. When examined from within, these foramina are found to be arranged in pairs, each pair corresponding to the point of exit of a spinal nerve. The foramen, which transmits the anterior root of each nerve, is separated from that of the posterior root by a narrow strip of fibrous membrane. Although not attached to any part of the vertebral canal between the foramen magnum and the sacrum, yet the spinal dura mater is sustained in its position by the prolongations of its substance over the nerves at each of the intervertebral foramina. It is also decidedly larger than would be necessary merely for the reception of the spinal cord; as, when pierced, a quantity of fluid escapes, and it becomes quite flaccid, to be again rendered tense by injecting water or air.
Cranial dura mater. The dura mater of the cranium differs in one essential point from that of the spine: namely, in that it forms a periosteum to the inner surface of cranial bones. It adheres closely to the whole interior of the cranium, and the free communication between the vessels of the dura mater and those of the bones serves materially to enhance the connexion between this membrane and the osseous surface. On the roofs of the orbits, the wings of the sphenoid bones, the petrous portions of the temporal bones, the margin of the occipital foramen, and opposite the sutures, the adhesion is very intimate.
The cranial dura mater is not a simple bag. From its internal surface partition-like processes pass inwards, which serve to separate certain subdivisions of the encephalon or brain. These are the falx cerebri, the tentorium cerebelli, and the falx cerebelli.
The falx cerebri is a process of fibrous membrane corresponding to the mesial plane, and lying in the great median fissure of the brain, where it separates the lateral hemispheres from each other. Its shape is falciform; its superior convex border corresponds to the frontal and sagittal sutures, and incloses the great longitudinal sinus; its inferior border is concave and much shorter than the superior, and corresponds to the superior surface of the corpus callosum, which connects the hemispheres of the brain. In front the falx is narrow, and almost pointed; it embraces the crista galli of the ethmoid bone, which appears to be inclosed between its layers. The falx cerebri contains within it, along its posterior border, a large vein, known as the inferior longitudinal sinus.
The tentorium cerebelli is continuous on each side with the posterior border of the falx cerebri. This process is nearly horizontal in direction. It forms a vaulted roof to a cavity, whose floor corresponds to the occipital fossæ, and in which the cerebellum is lodged. The posterior and outer edge adheres to the occipital bone, and to the posterior border of the petrous portion of the temporal. The occipital portion of this edge contains a considerable part of the lateral sinus, the portion adhering to the petrous bone containing the petrosal sinus. The anterior or inner margin of the tentorium is concave, and free in the greater part of its extent. It is attached by its anterior extremities to the anterior clinoid processes, to reach which it crosses the posterior border.
From the inferior surface of the tentorium cerebelli at its posterior edge, a short and thick fold of very slight depth descends to the posterior edge of the foramen magnum. This is the falx cerebelli. It corresponds to the median notch between the hemispheres of the cerebellum. Its anterior border is slightly concave. Two veins, called occipital sinuses, are contained in it.
Although the internal surface of the cranial dura mater usually presents the same smooth appearance as has been referred to in that of the spine, yet an exception is found along the great longitudinal sinus, in the occasional presence of small glandular bodies growing from the arachnoid membrane, and causing a peculiar cribriform appearance in the dura mater. These bodies, called glandulse or glands of Pacchioni, are in all probability not normal structures, but are rather morbid products of the arachnoid produced by continued cerebral excitement.
2. The Pia Mater. The pia mater, tunica intima vcl vasculosa, is the most internal membrane of those enumerated as belonging to the cerebro-spinal axis.
Pia mater of the spinal cord. This membrane stands in precisely the same relation to the spinal cord as the neurilema does to the nerves. It is composed almost entirely of white fibrous tissue, closely investing the cord, and supporting the minute blood-vessels which feed it. Not only does it form a complete sheath to the cord, but it likewise sends in processes which dip into the anterior and posterior median fissures of that organ. The spinous pia mater possesses considerable strength and density. When quite recent, it may be readily dissected off from the cord, its adhesion being through the medium of numerous exceedingly minute capillary vessels. On its exterior, the pia mater adheres to the visceral layer of the arachnoid membrane by means of a loose fibrous tissue.
Pia mater of the brain. In tracing the pia mater of the spine upwards, it will be found gradually to become thinner as it passes from the medulla oblongata to the hemispheres of the brain. Here it adheres closely to the whole surface of the brain, cerebellum, and connecting parts, numberless vessels passing from it into the nervous substance beneath. On the surface of the brain, it dips down into the furrow between the convolutions, and adheres to the superficial grey matter. At certain situations also, this membrane is continued into the ventricles of the encephalon, constituting the choroid plexuses.
3. The Arachnoid Membrane, intermediate between the two last described, is a great serous membrane pervading the entire cranio-spinal cavity. Its parietal layer adheres intimately to the inner surface of the dura mater, and its visceral to the outer surface of the pia mater. Like all serous membranes, it is composed of two layers, the interval between which is called the arachnoid bag or sac, and rarely contains fluid. Between the visceral layer of the arachnoid and the pia mater, is the sub-arachnoid cavity, usually including a considerable quantity of fluid. The object of this fluid is to protect the nervous centres with which it lies in immediate contact. By the interposition of a liquid medium between the nervous mass and the walls of the cavity in which it is placed, provision is made against a too ready conduction of vibrations from one to the other. Its composition, according to Lassaigne, is as follows:
- Water, 98.564
- Albumen, 0.088
- Osmazome, 0.474
- Chloride of Sodium and of Potassium, 0.801
- Animal matter and Phosphate of Soda, 0.036
- Carbonate of Soda and Phosphate of Lime, 0.017
- 99.980
Having thus treated in brief terms of the membranes of the cerebro-spinal axis, we come next to the essential structure of this part of the nervous system. This we shall consider under the heads of the spinal cord and of the brain or encephalon, the latter including the medulla oblongata, the mesocephalum, the cerebellum, and the cerebrum.
The Spinal Cord
The spinal cord occupies a large portion of the spinal canal, terminating inferiorly at a point, which in different subjects ranges between the last dorsal and the second lumbar vertebra. Below this point, the sheath formed by the dura mater contains that series of nerves known as the cauda equina. The entire length in the adult is from sixteen to eighteen inches. Its circumference measures twelve lines at the smallest, and eighteen at the most voluminous part. Its weight is said to be from the \(\frac{1}{19}\) to the \(\frac{1}{25}\) of that of the brain in the adult, and about the \(\frac{1}{40}\) part in the new-born infant. The actual weight of the spinal cord in the adult may be taken at a little over one ounce.
The consistence of the medullary substance of the spinal cord, when fresh, is much greater than that of the brain. The pia mater adheres very closely to its surface, like neurilema to a nerve. It is penetrated both on the anterior and posterior aspect by fissures, each of which corresponds to the median plane. They are separated from each other by a transverse bilaminate partition of white and grey matter, of which the grey layer is posterior. This serves to connect the equal and symmetrical portions into which the cord is divided by these fissures. The anterior of these fissures is deeper than the posterior. The two taken together seem to indicate the existence of two spinal cords, one for each side of the body, both presenting a perfect resemblance in form and structure.
On examining a transverse section of the spinal cord, we find that the interior of each lateral portion is occupied by grey matter disposed in a crescentic form, exactly similar in each, and connected by the grey commissure, a layer which extends between the two crescents, being attached nearly to the central point in each. This commissure forms a vertical plane of grey matter throughout the whole of the cord. The concavity of the lateral crescent is directed outwards. Their anterior extremities are thick, and separated from the surface of the cord by a considerable layer of white fibrous matter. The posterior extremities of the crescents are prolonged backwards and outwards in the form of a narrow horn, which reaches the surface of the cord. These posterior horns constitute on each side a natural boundary, between the two columns of which each lateral half of the cord consists. All in front of the posterior horns is called the antero-lateral column, comprehending the white matter forming the sides and front of the semi-cord, limited anteriorly by the anterior fissure, and posteriorly by the posterior roots of the nerves. The posterior column is situated behind the posterior horn of grey matter, and is separated from its fellow on the opposite side by the posterior fissure.
There are these four columns in the spinal cord, two antero-lateral and two posterior. The former constitute by far the larger proportion of the white substance of the cord, and they envelope the anterior obtuse portion or horn of the grey matter. The anterior roots of the nerves are connected with them, and the posterior roots adhere to them when the cord is split up along the plane of the posterior horn. The posterior columns are small, triangular in section, and placed in opposition with each other by their inner surfaces.
The spinal nerves. There is a pair of spinal nerves for each intervertebral foramen, and for that between the axis and occiput. There are thus thirty-one pairs of nerves having their origin from the spinal cord, this number being exclusive of the spinal accessory nerve, which is connected with the upper part of the cervical region. Each spinal nerve has its origin from the cord, by two roots, of which the anterior is distinctly inferior in size to the posterior. The ligamentum articulatum (a narrow longitudinal band on each side of the cord, and intervening between the dura mater and the pia mater, attached to the latter by tooth-like triangular processes) is placed between these roots. Each root passes out through a distinct opening in the dura mater. Immediately after its emergence a ganglion is formed on each posterior root, and the anterior root lies imbedded in the anterior surface of the ganglion, and involved in the same sheath, but without mingling its fibres with those of the ganglion. Beyond it, the nervous fibres of both roots intermingle, and a compound spinal nerve results. The trunk thus formed passes immediately through the intervertebral tube, and divides into an anterior (and usually larger) and a posterior branch, which are distributed to the muscles and integument of the trunk and the extremities.
The anterior roots derive their fibres wholly from the antero-lateral columns. Of these fibres, it is probable that some are continuous with the longitudinal fibres of the cord, and that others pass into the grey matter. The posterior roots adhere to the posterior part of the antero-lateral columns, and derive their fibres chiefly from that source. It is probable, though by no means certain, that the fibres of the posterior roots have a disposition similar to that described for the anterior, and that while some pass into the posterior horn of the grey matter, others are continuous with the longitudinal fibres.
In conclusion, the spinal cord may be said to be of a cylindroidal shape, slightly flattened on its anterior and posterior surfaces. At its inferior extremity it gradually tapers to a point. In the cervical region there is a swelling or enlargement, which begins a short distance beneath the medulla oblongata, and gradually passes into the dorsal portion, which is the smallest as well as the most cylindrical portion of the cord. This cervical enlargement begins opposite the third cervical vertebra, and ends about the third dorsal. About the ninth or tenth dorsal vertebra, the lumbar swelling occurs, occupying a space corresponding to about two vertebræ. The cervical swelling corresponds to the point at which the nerves of the upper extremities are given off, and the lumbar has the same relation to the lower limbs.
Pl. 137, fig. 3, spinal marrow and pons from the anterior surface: 1, dura mater; 2, ligamentum dentatum; 3, 3, 3, single dentations of do.; 4, a spinal nerve. Fig. 4, a portion of the spinal marrow represented on a larger scale: 1, dura mater; 2, ligamentum dentatum; 3, anterior root of a spinal nerve cut away; 4, do. entire; 5, a posterior root, with the ganglion; 6, anterior, 7, lateral furrow. Fig. 5, spinal marrow from behind: 1, posterior longitudinal furrow; 2, calamus scriptorum; 3, posterior column; 4, its division by a furrow into halves. Figs. 9, 10, 11, cross sections of the spinal marrow beneath the medulla oblongata.
The Encelphalon
The term encephalon is conveniently employed to denote the portion of the cerebro-spinal axis which is contained within the cavity of the cranium. Before proceeding to the description of the individual portions of the encephalon, it will be proper to premise some general considerations, borrowed from Tiedemann, having reference to its entire mass.
The average weight of the human brain amounts to about 48 ounces for the male, and 44 ounces for the female. The brain of men who have been distinguished for their intellectual attainments has often been found to exhibit a large size. That of Cuvier weighed 3 lbs., 11 oz., 4 dr., 40 gr. On the other hand, the brain of an idiot, fifty years old, weighed but 1 lb., 8 oz., and 4 dr.
The brain attains its full size, on an average, about the seventh or eighth year.
The brain of the new-born child is, relatively to the size of its body, the largest. The proportion is as 1:6. It decreases in proportion as man attains his full growth. Thus, in the second year the proportion of the brain to the body is as 1:14; in the third, 1:18; in the fifteenth, 1:24.
Although the female brain is absolutely smaller than the male, yet relatively to the size of the body it is usually larger.
1. Surface of the Encephalon. The brain, in horizontal projection, is seen to be of oval shape, the smaller end of which is directed forwards, the superior and lateral surfaces are convex, and have a smooth appearance, from the visceral layer of arachnoid being spread over them. When the membranes have been removed, the surface of the brain is seen to be impressed with numerous convolutions.
The superior surface is divided along the median plane into two equal and nearly symmetrical portions by a vertical fissure, which receives the great falx of the dura mater. In front and behind, this fissure completely divides the central lobes. In the middle, the fissure is interrupted by a horizontal lamina of white fibres, called the corpus callosum, the great commissure of the cerebral hemisphere. The inferior surface of the brain presents three segments each on a different plane, and corresponding with the three fossæ of the cranium. The anterior segment, and the one on the highest level, correspond to the anterior fossa of the cranium, and rest upon the roofs of the orbits. The continuation of the anterior median fissure separates its right and left portions, this distinction being rendered more complete by the attachment of the falx to the crista galli of the ethmoid. In a distinct sulcus, parallel to and immediately on each side of the longitudinal fissure, we find the olfactory process or nerve. A curved fissure of considerable depth, called the fissure of Sylvius, is the posterior limit of each anterior segment. The fissure of Sylvius corresponds on each side to the posterior concave edge of the ala of the sphenoid bone, which is received within it. Commencing from within, at a triangular flat surface (locus perforatus anticus), at the posterior extremity of each olfactory process, it proceeds outwards and curves backwards, its convexity directed forwards to the lateral surface of the brain. It is of considerable depth, especially at its internal extremity, and like all fissures of the brain, is lined by pia mater. The island of Reil is found at the bottom of this fissure, projecting from its floor as a small insulated lobe, bounded by a bifurcation of the fissure.
The middle segment, which lies immediately behind the fissure of Sylvius, is on a plane much lower than the anterior, and corresponds on each side to the deep and hollow median fossa of the cranium. It consists of two lateral, very convex lobes, known as the middle lobes of the brain, which are separated from each other by a deep depression. These lobes, which are distinctly defined in front by the fissure, have no exact boundary behind, but pass off very gradually into the posterior lobes of the hemispheres, as may be seen by raising up the cerebellum.
Commencing at the anterior fissure and passing backwards we shall perceive the following parts. This fissure is limited by the anterior fold or reflexion of the corpus callosum; behind this is a thin layer of a greyish color which principally constitutes the floor of the third ventricle, and is known as the tuber cinereum. The pituitarg process is continuous with it, being probably its extension, and is a hollow process of nervous matter above the sella turcica by which the brain is in a measure tied to the pituitary body.
Immediately in front of the pituitary process, the union of two white bands, which form lateral boundaries to a large portion of the tuber cinereum, the optic tracts, takes place along the median line. This forms the commissure of the optic nerves from which these nerves diverge. Behind the pituitary process, the tuber cinereum extends back to two small and very white bodies called corpora mammillaria or albicantia.
Behind the mammillary bodies, we find a deep depression, lying between two thick processes of fibrous matter, which pass from below upwards and outwards, expanding as they advance, and upon which each hemisphere is sustained like a mushroom on its stalk. These are the crura cerebri, the peduncles of the cerebral hemispheres. The depression separating them is the intercrural space. The nervous matter forming the floor of this space is of a greyish color and known as the pons Tarini. The third pair of nerves emerges from the interpeduncular space.
The inner margin of each middle lobe of the brain is separated from the corresponding crus cerebri by a fissure which passes from behind forwards, and terminates in the fissure of Sylvius. Backwards this fissure is continuous with the transverse fissure separating the cerebrum from the cerebellum, and corresponding to the posterior edge of the corpus callosum. The continuity thus established between these three series of fissures constitutes the great cerebral or transverse fissure.
The posterior segment, as occupying the posterior fossa of the cranium, is on a level considerably below that of the middle segment. A part worthy of especial notice is the pons Varolii, which is situated immediately behind the interpeduncular space, the crura cerebri appearing to emerge just above its anterior border. From its posterior edge the medulla oblongata extends downwards and a little backwards, occupying a notch or depression between the lobes of the cerebellum. The fibres of the pons are seen passing outwards and backwards into each hemisphere of the cerebellum, forming the inferior layer of each crus cerebelli.
2. Dissection of the Encephalon. If we make a horizontal section of one hemisphere, nearly on a level with the corpus callosum, we shall perceive what is known as the centrum minus ovale, a mass of white fibrous substance surrounded by an irregularly undulating line of grey; a second horizontal section passing through both hemispheres on a level with the corpus callosum presents the centrum magnum ovale, a line of grey substances surrounding the central mass of white. The corpus callosum, or superior cerebral commissure, will now be seen in the middle line of the cerebrum, between three and four inches long, marked by two or three raised longitudinal lines nearly parallel to each other (the raphe), from these, several transverse lines pass to either side. The posterior end of the corpus callosum is bent downwards above the transverse fissure, and is continuous with the fornix and hippocampi; anteriorly it is continued into the anterior lobes: in the middle it joins the tuber cinereum and the optic commissure. It connects the white fibrous substance of both hemispheres, and covers like an arch the lateral ventricles, the septum lucidum, and the fornix.
On dividing the corpus callosum at a little distance from either side of the raphe, the lateral ventricles or cavities of the brain will be opened, one on each side, and separated by the septum lucidum. This consists of four laminæ on each side: 1. The lining membrane of the ventricle; 2. A thin grey layer; 3. A compact white fibrous layer; 4. A delicate membrane which lines the small cavity existing in it, and termed the fifth ventricle.
The lateral ventricles extend from the middle of the brain into the anterior and posterior lobes, also into the inferior part of the middle lobe; each has, therefore, three cornua. The anterior cornu is bounded superiorly and laterally by the corpus callosum, and inferiorly by the large extremity of the corpus striatum. The middle or body of each ventricle is bounded superiorly and externally by the corpus callosum; internally by the septum lucidum, and inferiorly by the posterior extremity of the corpus striatum, the lamina cornea, the tsenia semicircularis, the optic thalamus, the choroid plexus, and the fornix. The posterior cornu is bounded superiorly and laterally by white substance, and inferiorly by the hippocampus minor. The inferior cornu is bounded superiorly by the optic thalamus and corpus striatum; inferiorly by the hippocampus major and corpus fimbriatum or tænia hippocampi, over which the choroid plexus is folded.
In making a brief individual reference to the different bodies observed in each lateral ventricle, we commence with the corpus striatum, a pear-shaped eminence situated in the anterior horn, the obtuse extremity directed forwards and inwards. Posteriorly the body is apparently prolonged backwards into the inferior cornu of the lateral ventricle by a long tapering process, which terminates there. Internal and posterior to the corpus striatum is the optic thalamus, a gangliform body of greyish color. These two bodies are separated from each other by a superficial groove, in which lies a delicate band of fibrous matter, the tænia semicircularis, which is covered by a lamina of horny-looking matter, the lamina cornea.
The choroid plexus is a fold of thin and very red vascular membrane derived from the pia mater, which enters the inferior cornu by the great cerebral fissure, and ascending, turns inwards just behind the septum lucidum and anterior pillars of the fornix, and unites with its fellow of the opposite side, covering and nearly concealing from view the optic thalamus.
In the posterior cornu, there is seen in its internal wall a projection upwards of one of the convolutions, to which the name of hippocampus minor has been given. It is traversed by a deep furrow. In the descending horn is a remarkable prominence, the hippocampus major, projecting into it from the inferior wall and following the curve of the horn. Beneath this is a peculiar grey matter, connected with the hippocampus, known as fascia dentata. A thin margin from the fornix which overlaps the hippocampus is called the corpus fimbriatum.
The fornix is a white, fibrous, triangular arch or vault, convex above, situated horizontally beneath the corpus callosum and septum lucidum; it lies on the velum interpositum and choroid plexuses, and over the third ventricle. The base, posteriorly, arises by two long flat bands (the posterior pillars or crura), one from either side, by three roots, from the hippocampus major and minor and from the tsenia hippocampi; these crura unite to form the body of the fornix, which bending forwards divides into two short round cords, the anterior pillars of the fornix. The inferior surface of the fornix is marked posteriorly with several fine oblique lines (lyra or corpus psalloides); although described as single it is really double, and divisible throughout except where the lyra unites opposite sides. It may be called the great inferior commissure of the cerebrum, the corpus callosum constituting the great superior commissure. The anterior pillars of the fornix bound a space in front, through which the lateral ventricles communicate with each other through the foramen commune anterius.
The third ventricle. If the fornix be divided transversely at about its middle, and the segments reflected, the velum interpositum being removed, a fissure known as the third ventricle, and situated between the optic thalami, will be exposed. Anteriorly and between the anterior pillars of the fornix this fissure is limited by a band of white matter called the anterior commissure. At its posterior extremity the third ventricle becomes much contracted in all its dimensions, and is continuous with a canal (aqueductus Sylvii) which leads to the fourth ventricle. The roof of the third ventricle is formed by the velum interpositum.
The pineal gland. This body, rendered famous by the vague theory of Descartes, which viewed it as the chief source of nervous power, is placed just behind the third ventricle, resting in a superficial groove which passes along the median line between the corpora quadrigemina. It is of a greyish color, heart-shaped, with the apex directed backwards and downwards. A process from the deep layer of the velum interpositum envelopes it and retains it in place. From each angle of the base there passes off a band of white matter to the inner surface of each optic thalamus, called the peduncles or habenæ of the pineal gland. The only connexion with the brain is by means of these habenæ. In the adult, grains of sandy matter are usually found in the pineal gland, which are mostly collected in a cavity towards its base; sometimes, however, situated on the surface.
The soft commissure is a lamina of light grey matter, situated in the third ventricle, and extending between the optic thalami of opposite sides. It forms a transverse horizontal plane dividing the ventricle into two portions.
We come next to consider that part of the brain which lies intermediate to the cerebrum, cerebellum, and medulla oblongata, and conveniently termed the mesocephalon. The pineal body rests upon its upper surface; but from its internal relation to the third ventricle and optic thalami, we found its description with them most convenient.
3. The Mesocephalon. The limits of the mesocephalon cannot readily be defined, as it is continuous with the crura cerebri above, with the crura cerebelli behind, with the medulla oblongata below, and with the cerebellum itself above and behind. Many treat of it as one mass with the medulla oblongata. We shall consider it as composed of the tubercula quadrigemina and the pons Varolii.
The corpora, or tubercula quadrigemina, are four eminences seen immediately behind the third ventricle. A transverse furrow separates them into an anterior, the nates, and a posterior pair, the testes; a longitudinal furrow along the median line divides the right and left pairs from each other. The pineal body rests in the anterior extremity of the longitudinal depression.
The posterior crura of the corpora quadrigemina are connected with the cerebellum by two columns of white matter, one of which passes into the central white substance of each cerebellar hemisphere; these are the processus cerehelli ad testes. They enter into the formation of the crura cerebelli. The interval between the two processus cerebelli is occupied by a horizontal stratum of nervous matter called the valve of Vieussens, or of the fourth ventricle.
The pons Varolii, or great commissure of the cerebellum, is somewhat square, and placed obliquely on the cuneiform process between the cerebrum and the cerebellum. The fourth ventricle, the aqueduct of Sylvius, and the corpora quadrigemina are on its superior and posterior surface. Its superior extremity receives the crura cerebri, which it surrounds like a ring, and is hence sometimes called the annular protuberance; the crura cerebelli are attached to its sides, and the medulla oblongata to its lower extremity, from which it is distinguished by a deep groove. Its surface is white and fibrous: the superficial layers of fibres on its inferior surface run transversely from the inferior surface of one crus cerebelli to the other.
4. The Cerebellum. The cerebellum is seen on removing the posterior lobes of the cerebrum and dividing the tentorium. In size and weight it bears to the cerebrum a ratio of about as one to eight; the average weight of the cerebrum being two pounds and a half, that of the cerebellum amounting to about four ounces and a half It is somewhat different in form from the cerebrum, being oval transversely, and raised in the centre, where its right and left hemispheres are united. Like the cerebrum it is composed of white substance internally and of grey upon its surface, upon which it is marked by a great number of parallel narrow lines, running semicircularly convex posteriorly; these are fissures to the bottom of which the pia mater descends, the arachnoid membrane passing over them. Some lines called primary pass very deep into the cerebellum, and divide it into lobes: secondary lines, more superficial, divide these into lobules.
The cerebellum presents for examination a superior and inferior surface, a convex border or circumference, and a median notch behind and before. The posterior notch is very deep. It receives the falx cerebelli and the inferior occipital crest, and extends close along the "under surface as far as the back of the medulla oblongata. This extension is called the valley or the purse-like fissure. The anterior notch is broad, overlaps the fourth ventricle, and embraces the central protuberance and tubercula quadrigemina. These two notches mark a division of the cerebellum into right and left hemispheres, the circumference of each of which is deeply indented by the horizontal fissure.
The superior surface of the median portion of the cerebellum is known as the superior vermiform process. Its anterior terminal laminæ form the valve of Vieussens. On the inferior surface the hemispheres are much more convex than on the superior. The median portion consists of a series of laminæ following a transverse direction, those in the centre being of greater transverse extent than those at either extremity, and constituting the inferior vermiform process. These two processes, which have thus received distinct names, are really but one, and might be properly termed the median or primitive lobe of the cerebellum. In the lower orders of vertebrata this median lobe alone exists, the lateral portions increasing with the ascent in the organic scale.
The cerebellum may therefore be considered as divided into the median lobe and two lateral hemispheres. The hemispheres present the lines or sulci already referred to, on their superior surface, dividing them into lobes and lobules. We can only briefly indicate these divisions in a general survey of the entire cerebellum as follows:
a. The cerebellum is divided into three parts, viz. right and left hemispheres, and middle or primary portion, b. Each of these is subdivided by the horizontal groove into superior and inferior, c. The upper surface of each hemisphere presents two lobes, the anterior or square, and the posterior or semilunar. The two former are connected by the tortuous transverse laminæ of the superior vermiform process, and the two posterior by those forming the floor of the posterior notch, d. The median portion presents the single or azygos superior median lobe or vermiform process, e. The interior surface of each hemisphere presents five lobes. Most anterior and distinct from the hemisphere are: first, the flocculus or pneumogastric lobule, connected to its fellow and to the nodule by the inferior medullary velum; second, the tonsihc lobe or amygdalar, on the side of the ventricle, and connected to the opposite through the uvula or spigot; third, the digastric; fourth, the gracilis; fifth, the semilunar, which is joined to its fellow by the convex transverse laminæ at the bottom of the posterior notch; sixth, the inferior median lobe, or vermiform process, presents from before backwards three lobules; the nobule most anterior, next the uvula or spigot, and posteriorly the pyramid.
The fourth ventricle is a lozenge-shaped cavity, situated in the upper and posterior part of the medulla oblongata, and formed by the separation of its postero-lateral columns (corpora restiformia). The cerebellum contributes to inclose it by means of the anterior laminæ of the superior vermiform process and the valve of Vieussens, and below and behind by the inferior vermiform process.
5. Medulla Oblongata. The medulla oblongata, or spinal bulb, is that conical portion of white substance which extends from the lower margin of the pons Varolii to the spinal cord, on a level with the ring of the atlas. Its upper end or base, though apparently limited by the pons, is prolonged upwards through it to the crus cerebri of each side. Inferiorly, there is no distinction between it and the spinal cord posteriorly or laterally. It presents an anterior and posterior median fissure, which divides it into two symmetrical portions, each of which is marked by three grooves and four convex eminences, viz. the anterior pyramid, the corpora olivaria, the corpora restiformia, and the posterior pyramid.
The posterior fissure is continuous with that of the spinal cord. It is narrow, deep, and lined by the pia mater. The anterior fissure, the continuation of the spinal, is broader but shallower, and lined by transverse commissural fibres. Nearly an inch below the pons this fissure is interrupted by the decussating fasciculi, three or four in number, which ascend obliquely inwards from the lower end of each pyramid to the opposite one, interlacing or interdigitating with each other.
The anterior pyramids are two narrow, convex, white bands, about an inch long, small inferiorly, and partially united by the decussating fasciculi. They appear to be the direct as well as decussating medium of communication between the anterior fibres of the cord, the mesocephalon, crura cerebri, corpora striata, and cerebral hemispheres.
The corpora olivaria are smaller and shorter than the pyramids, are external and posterior to these, and separated by a groove both from them and from the restiformia. They only exist in man and quadrumana. White and fibrous externally, when divided they present a mass of grey neurine called olivary ganglion or corpus dentatum.
Corpora restiformia, or the inferior peduncles of the cerebellum, are two thick longitudinal white cords on each lateral and posterior surface of the medulla, separated from the olivaria by a groove, in which the roots of the eighth pair of nerves are lodged. Each of these connects the spinal cord and the medulla oblongata with the cerebellum.
Posterior pyramids are two long narrow columns which extend on each side of the posterior fissure of the cord to its lower extremity. They are seen on each side of the calamus scriptorius in the lower part of the ventricle, and terminate abruptly. By their deep surface they appear continuous with the posterior part of the olivary tracts.
Pl. 137, fig. 1, view of the brain from above. Fig. 2, base of the brain: 1, continuation of the great median fissure along the inferior surface of the brain; 2, anterior cerebral lobes; 3, fissura Sylvii; 4, middle cerebral lobe; 5, commissure of the optic nerves; 6, tuber cinereum, with the process proceeding from the pineal gland; 7, corpora mammillaria; 8, crura cerebri: 9, pons Varolii; 10, cerebellum; 11, limit of the superior lobe of the cerebellum; 12, the flocculus; 13, inferior vermiform process; 14, anterior pyramids; 15, olivaria; 16, restiformia; 17, olfactory nerve; 18, optic nerve; 19, motor oculi; 20, trochleator; 21, trigemini or fifth pair; 22, abducens nerve; 23, facial and auditory nerves; 23′, glosso-pharyngeal and pneumogastric nerve; 24, accessory nerve; 25, lingual nerve. Fig. 3 5, lingual nerve; 6, glosso-pharyngeal, pneumogastric, and accessory nerves; 7, facial and auditory nerves; 8, trigemini; 9, abducens oculi; 10, optic nerve; 11, cauda equina; 12, lumbar enlargement of the spinal cord; 13, cervical do.; 14, medulla oblongata; 15, anterior spinal fissure; 16, lateral do.; 17, olivaria; 18, pyramids; 19, pons; 20, crura cerebri. Fig. 6, medulla oblongata; 1, fibres separating to inclose the corpora olivaria; 2, lateral fibres; 3, point where these decussate; 4, posterior fibres of the olivary column; 5, 5′, pyramids: 6, 6′, their continuations into 7; and 7, the crura cerebri. Fig. 7, cross section of the corpora olivaria: 1, their cortical substance; 2, corpus dentatum; 3, medullary substance. Fig. 8, vertical section of the pons Varolii, and of the medulla oblongata. Fig. 12, cross section at the point of decussation of the pyramidal columns. Fig. 13, cross section of the central portion of the medulla oblongata. Fig. 14, cross section at the point of union between the medulla oblongata and the pons.
Psychological Relations of the Brain
Numerous experiments have been made by accomplished physiologists to determine the modus operandi of the brain as the source of voluntary action and the recipient of sensitive impressions. We may point to a few general conclusions as tolerably well established by careful research, although still open to examination. They are as follows:
- The vesicular matter of the brain is the source of nervous power. In mental actions it is the part immediately associated with changes of the mind, whether in the working of the intellect, or in the exercise of the will, or in the perception of sensitive impressions.
- In simple operations of thought, as in the exercise of the reasoning powers, or of those of the imagination, the convolutions of the brain are immediately engaged. We do not say that material changes give rise to the mental actions, but rather that the changes of the immaterial mind and those of the vesicular matter of the convolutions are simultaneous.
- The simple exercise of the will for a voluntary movement is probably connected with the corpora striata.
- The mere reception of sensitive impressions is connected with the optic thalami and the superior layers of the crus cerebri.
- Mental emotions affect the posterior and superior part of the mesocephalon.
- The cerebellum is the regulator of the locomotive actions.
The harmony of the cerebrum is affected by various causes, whose influence is then exhibited in abnormal mental or bodily phenomena. A violent concussion or a severe electrical shock may either produce immediate death, or else cause stupefaction, loss of memory, wandering of mind; turning the body rapidly round causes vertigo. The excessive use of ardent spirits or narcotics may effect the same result, delirium, insanity, and lethargy following in their train. The poet may have his inspiration excited and increased by wine, the use of which would only blunt the calm reflection of the mathematician.
These brief indications may serve to introduce the subject of Phrenology or Cranioscopy, the science which professes to decide upon the mental peculiarities of man and animals, from the form and relations of certain portions of the exterior of the skull.
This subject was first elaborated by Gall, born at Tiefenbrun in Swabia, March 9th, 1757. For a time settled in Vienna as a physician, he subsequently moved to Paris, where he died August 22d, 1828. He well knew that it was the brain and not the skull that was connected with the mental phenomena, yet as it was impossible to have access to the former in the living individual, he took the latter as its measure, assuming the exterior of the skull to be an exact model of the inequalities on the surface of the brain. Associating himself with Spurzheim, a former pupil, Grail endeavored to bring his hypothesis to the rank of a well established theory. In the following article we present the principal features of their science.
Phrenological System of Gall Spurzheim
The mental powers of an animal are numerous in proportion to the complexity of its brain; the remarkable diversities in the structure of the brain in different animals stand in immediate relation to the special variations in their mode of life and general functions.
In all organized beings different phenomena presuppose different organs; thus the different functions of the brain imply different organs.
One animal possesses inclinations and instincts which are wanting to another; this is only explicable on the supposition that every special function of the brain is limited to a particular portion of it.
The gifts and peculiarities found in all individuals of the same species exist in different degrees in the different individuals; this can only be explained by a difference in the activity of the different organs regulating these peculiarities.
In the same individuals the different original gifts are found in very different degree; this could not be were not each original mental peculiarity dependent on a special organ.
The essentially different functions of the brain never present themselves simultaneously either in man or in animals: some are constant, while others acquire a maximum development, either with the age of the subject, or the season of the year. This cannot be explained on the supposition that all functions are dependent on a single organ.
A too long continued exercise of the mind does not enfeeble or weary all the mental powers equally: the fatigue is only partial, and rest can be attained by changing the subject of study, without the necessity of entire cessation from labor. This would be impossible if the whole of the brain were concerned in any species of mental application. Certain mental and moral powers may be destroyed, blunted, or heightened by disease, wounds, &c., while others remain entirely unaffected by the same causes: this would be incomprehensible on the supposition that the brain is a single uniform organ adapted equally to all functions.
Little exception can be taken to the postulates of Gall as above presented: the case is different, however, in respect to the conclusions which he attempts to draw from them. According to him all the organs of the mind lie on the surface of the brain in the different convolutions, and they are more or less depressed or elevated, are larger or smaller as their functions are exercised with greater or less energy. These different developments of the brain are supposed to be impressed on the surface of the cranium, and externally visible. To this, however, positive facts of anatomy and physiology are decidedly opposed. According to the present state of our knowledge of the functions of the brain, it is not upon the surface that we are to seek for the seat and impress of mental characteristics, but rather on the walls of the ventricles whose varying features are not exhibited on the surface of the brain, much less on the exterior of the cranium. The most accurate anatomico-physiological investigations lead to the conclusion that in men of high mental endowments the regions of the posterior and inferior cornua of the lateral ventricles are especially developed, yet these are so entirely concealed from view as to yield no definite conclusions in the unopened cranium.
On pl. 120, figs. 15, 16, 17, the organs as originally established by Gall will be found indicated by the figures 1 to 27, as follows:
1. Sexual love. 2. Love of children. 3. Capacity for communicating instruction. 4. Knowledge of the relative positions of objects. 5. Knowledge of persons. 6. Sense of color. 7. Sense of melody and harmony. 8. Talent for calculating. 9. Facility in expressing thoughts in writing. 10. Fluency of speech. 11. Power of construction. 12. Friendship; attachment; fidelity. 13. Courage; power of self-defence; tendency to bullying. 14. Disposition to destroy life. 15. Tendency to conceal mental emotions. 16. Propensity to steal; to acquire property, &c. 17. Pride; arrogance; self-respect. 18. Love of approbation; vanity. 19. Cautiousness; prudence; excessive timidity. 20. Power of comparison, or of discovering analogies. 21. Metaphysical acumen; tracing the relations of cause and effect. 22. Wit; disposition to mirth. 23. Poetic feeling; ideality; love of the beautiful. 24. Benevolence of disposition; good humor. 25. Religious feeling. 26. Firmness; obstinacy. 27. Mimicry; power of imitation.
The regions of the skull marked ? were left unnamed by Gall.
The hypothesis of Gall, which for a time counted numerous adherents, was subsequently almost entirely forgotten, and only resuscitated in more modern times by the labors of English and American investigators. Although the general principles remained the same, the number of organs was increased from twenty-seven to thirty-six, and the name of the science changed from Cranioscopy to that of Phrenology.
Some phrenologists, with Noel, assume the following six regions as connected with the mental faculties: 1. The posterior basilar region, containing the cerebellum, and supposed to be the seat of the instinct of reproduction. 2. The lateral basilar region, the region of the ear; the seat of the inferior, selfish feelings; the propensities to self-aggrandizement, distinction, &c. 3. The posterior region of the head above the cerebellum, the seat of social qualities, love of children, attachment, fidelity, &c. 4. The region of the vertex, or crown of the head, the seat of the higher egotistical feelings, as self-esteem, love of approbation, &c. 5. The anterior superior portion of the head, the seat of the higher moral and religious sentiments, as benevolence, veneration, firmness, conscientiousness. 6. The forehead, the seat of the intellectual organs, the perceptive being situated in the lower part, the reflective above.
We shall now, in conclusion, present the order in which the different mental faculties are mapped out by phrenologists of the present day, referring to pl. 120, figs. 18–21.
- Propensities or Instincts.
- Amativeness: lies between the occipital condyles.
- Philoprogenitiveness: lies above the middle of the cerebellum. Its form varies; in some it is an oval elevation, as in females; in others it is more elongated.
- Inhabitiveness: beneath Self Esteem. It produces the desire of permanence in place.
- Concentrativeness: lies between Philoprogenitiveness and Inhabitiveness. The power of concentrating all the faculties on one point.
- Adhesiveness: on each side of the preceding. Attachment, friendship, love of society.
- Combativeness: situated on each side, at the inferior posterior corner of the parietal bones.
- Destructiveness: immediately above the external ear, extendmg on each side.
- Secretiveness: immediately above Destructiveness. When the two last organs are highly developed, the cranium acquires a peculiar shape in the extension or prominence of the inferior lateral portion.
- Acquisitiveness: situated at the anterior inferior angle of the parietal bone.
- Constructiveness: situated at the inferior lateral portion of the frontal bone, in the vicinity of the sphenoidal suture.
- Sentiments.
- Self-Esteem: lies on the posterior portion of the top of the cranium; when strongly developed, it constitutes the vertex, or highest part of the head.
- Love of Approbation: on each side of the preceding.
- Cautiousness, running into prudence and timidity: a little below the middle of the parietal bone.
- Benevolence, the source of compassion: lies on the upper part of the frontal bone.
- Veneration: tendency to respect what is great and good; lies between Firmness and Benevolence.
- Firmness: placed in the posterior portion of the coronal suture.
- Conscientiousness: anterior to Hope, lateral to Firmness.
- Hope: on either side of Veneration.
- Wonder, Credulity: on one side of Benevolence.
- Ideality: love of the beautiful, desire for excellence; on one side of Wonder.
- Imitativeness: next to Benevolence.
- Intellectual Faculties.
- Individuality: takes cognisance of existence and simple facts; lies in the lowest part of the forehead, immediately above the root of the nose.
- Form: idea of external shape; situated at the interior angle of the orbit.
- Size: gives the idea of space, and enables man to appreciate distance and dimension.; placed at the interior angle of the superciliary arch.
- Weight: communicates the perception of momentum, weight, and resistance, and aids equilibrium: lies behind the preceding, on the superciliary arch.
- Color: gives perception of colors and their harmonies; lies a little beyond the middle of the superciliary arch, next to the preceding.
- Locality: idea of relative position; placed on each side, at the middle of the inferior edge of each frontal bone.
- Number: above the outer angle of the eyebrows.
- Order: the love of physical arrangement; lies next to Color, and forms the outermost organ in the superciliary arch, bordering externally on Number.
- Eventuality: takes cognisance of occurrences or events; lies in the middle of the forehead.
- Time: borders on Sound, Eventuality, Locality, and Wit.
- Tune: a considerable development enlarging the anterior portion of the forehead, and giving to it an angular shape: said to be very conspicuous in Liszt. It appears to have been pyramidal in Gluck and Haydn, and rounded in Mozart, Yiotti, Zumsteeg, Dussek, and Crescentini.
- Language: situated on the anterior inferior portion of the anterior lobe of the brain, immediately above the vault of the orbits. In proportion to its development, it depresses the vault of the orbit, forcing out, and giving a fulness to the eyes.
- The Intellectual Reflective Faculties.
- Wit: lies beneath the inferior external portion of Wonder.
- Comparison: lies beneath the organ of Benevolence. This and the next organ sometimes constitute a single lump.
- Causality: traces the relation of cause and effect, and the dependence of phenomena; lies beneath Imitation, and borders on Wonder, Benevolence, Comparison, Eventuality, and Time.
We may characterize the instinct of nourishment, and the love of life, as acquired faculties. Their supposed locations are indicated by ⊕ and + on fig. 19. The regions marked ? are uncertain.
The More Modern Methods of Cranioscopical Investigation

The first point to be ascertained is as to the general size of the cranium to be examined, whether it be large, of medium size, or small. We next consider the relative extent of the principal regions of the cranium as already referred to, going into an estimate of the individual organs present, with reference to their length, breadth, and thickness; by this means we obtain an idea of their mutual relations. The head in question is next to be examined in profile, dividing it into two portions by means of a vertical line (pl. 120, figs. 1, 2, a b), which extends from the opening of the external ear a, to the central point b, of the upper part of the head, corresponding to the intersection of the frontal and sagittal sutures. The posterior surface is the occipital, and the anterior the frontal region; the extent of each is next to be determined. In fig. 1, the occipital region a b d predominates over the frontal a b c; the reverse is seen in fig. 2. The former condition is the more common, indicating a preponderance of the animal over the intellectual in man. In each figure now draw lines a c, a f, a b, a d, from the external auditory meatus; these lines, by their different lengths, will indicate the different degrees of cerebral development in the different planes of intersection. Next examine the length c d, from the occipital to the frontal region, as also the height of the head a b, from the ear to the vertex. Then divide the head, with respect to its height, into two regions, by means of a horizontal line c d, from the middle of the frontal region to the point of union of the parietal bones and the occiput. The portion below this bone is called the basilar region, that above it the coronal. Of these two regions, the former will usually be found most highly developed; another indication of the preponderance of the animal. A line e f drawn from the outer corner of the eye, vertical and parallel with a b, indicates the degree of development of the brain in the forehead proper; as also the volume of its lower portion e c, with that of the upper c f, The former of these bears reference to the perceptive faculties, the latter to the reflective.
Finally, take the entire circumference of the head into consideration, and compare the height with the breadth, by which means we shall obtain the relation between the lateral and the superior region. The usually greater development of the lateral region in proportion to that of the fore part of the head, again points to the preponderance of the animal in man. We may next proceed to the consideration of the single organs situated in each of these regions.
In the frontal part of the head lie the intellectual faculties, the perceptive being inferior and the reflective superior. All the rest of the head belongs to the feelings; the basilar and lateral portions to the instincts, the vertical to the feelings. The part adb of the region of the vertex deserves especial mention, on account of the influence which the organs situated in it exercise upon the operations of all the rest, exciting and communicating a greater degree of energy to them. This part of the head, in connexion with a well developed frontal and vertical region, imparts strength both to the intellectual and the moral faculties, while in connexion with a high development of the basilar region it invigorates the animal impulses.
Quite recently Cams has endeavored to establish Cranioscopy on a more scientific basis than hitherto. He starts with the principle that the skull consists of three vertebra?, and that these three vertebræ correspond to the three divisions of the brain, anterior, middle, and posterior; which in turn stand in strictest relation to the three directions of spiritual activity, the intellect, the sensibility, and the will. He made use of every opportunity in his power to obtain measurements of the most diverse heads, comparing, too, a great number of skulls and plaster casts, and from his different examinations attained to the following noteworthy results. We may remark that the measurements given are in the German inch, which is slightly larger than the English.
He never found that among men in whom there existed a deficient development of the anterior or frontal vertebra (in height less than 4 inches 6 lines measured from the opening of the ear, and a breadth of forehead less than 4 inches) there was any decided intellectual development. On the other hand, in an extensive series of remarkably intellectual individuals he found the volume of the frontal vertebra to be always considerable (5 inches to 5\(\frac{1}{2}\) high and 4\(\frac{1}{2}\) to 5 inches broad). As instances Cams adduces Kant, the great metaphysician: Ehrenberg, the naturalist; Retzius of Stockholm, the anatomist; Von Raumer, the historian; Von Lindenau, the statesman; the artists, Ranch (5 inches 4 lines high, 4 inches 7 lines broad), Bendemann, and Thorwaldsen (5 inches 2 lines high, 4 inches 8 lines broad); the poets, Schiller, Goethe, and Tieck: in all these there was a striking anterior development. In the head of the Italian philosopher Nobili alone did he find so slight dimensions as a height of 4\(\frac{1}{2}\) inches, and a breadth of 4\(\frac{1}{2}\), and in his case the whole skull was very delicately organized, the bones of the forehead very thin, with a considerable breadth of the tympanic vertebra (5\(\frac{1}{2}\) inches).
In a series of measurements of the heads of very intelligent and highly gifted women, he never found so great a height of forehead as in eminent men. The greatest size occurred in the authoress Mrs. Austin.
Measurements of the middle and posterior regions of the head gave frequent occasion to recognise the relation between them and the sensibilities and will. With a middle region of only 5 inches or less, the skull always belonged to a low depraved nature. Two convicted thieves exhibited a height of 4 inches 10 lines and 5 inches 1 line, with a breadth of 5 inches 2 lines. In the skulls of various savage tribes, as New Hollanders, Botocudas, Guaraguanas, Aleutians, Negroes, Baschkirs, &c., the height was only 4 inches 5-10 lines, and the breadth 4 inches 1–8 lines. On the other hand, in poets, artists, and savans, the height amounted to 5 inches 4–7 lines, and the breadth to 5 inches 5–9 lines. With respect to the hind part of the head, its height was always characteristic of energy of action; whether this was spiritual or corporeal in its nature, depended upon the greater or less development of the region of the intellect. Thus a very muscular Arabian springer was distinguished by an enormous height of occipital vertebra (4 inches 5\(\frac{7}{8}\) lines); while in other more spiritually gifted persons of great power of will it amounted to 3 inches 7 lines to 5 inches, by 4 inches 4–5 lines (in Ole Bull, 3 inches 11 lines; in Thorwaldsen, 4 inches 3 lines).
Measurements of the middle head of females differed less from those of males than was seen in the case of the fore or hind part of the head; in general they indicated a more or less predominant sensibility. The comparison of the heads of the eminent German actresses, Schroeder, mother and daughter, was highly remarkable in this respect. The former, sedate, measured, and stately in her performances, had a middle head measuring 4 inches 10 lines in height, and 5 inches 1 line in breadth, with a hind head of 4 inches 4 lines in height; the latter, who was also a great singer of wonderful creative fancy, had a middle head of 5 inches in height and 5\(\frac{1}{2}\) inches in breadth, with a height of but 3 inches 11 lines for the hind head. A pair of female criminals, one a poisoner, the other a child murderer, exhibited a height of 4 inches 5–10 lines, with a common breadth of 5 inches 3 lines for the middle head. The height of the hind head in females was generally about 4 inches, never over 4 inches 4 lines, while in males it may amount to 4 inches 8 lines, thus corresponding to the greater weakness of the former sex.
With respect to the import of varying height and breadth in the cranial vertebræ, Carus came to the conclusion, that a greater breadth in the anterior cerebral mass, and in the sincipital vertebra, was connected with a greater tendency to a philosophical intellect. In the middle portion of the head, too, variations in height and breadth appear decidedly to run parallel with a more or less subjective direction of mind. In the occipital vertebra, if the height seems more to keep pace with the motive energies, the breadth is more in harmony with sexual characteristics.
In illustration of the above developments, pl. 120, fig. 3, represents a cast of the head of Napoleon; fig. 4, that of Tiedge; fig. 5, of Kant; fig. 6, of Talleyrand; fig. 7 represents the skull of Schiller; fig. 8, that of a Greenlander; fig. 9, that of a suicide; fig. 10, that of a poisoner; fig. 11, that of a Cretin; fig. 12, that of an idiot; fig. 13, that of a brown sajou ape; fig. 14, that of a Grison ape.
Anatomy of the Nerves
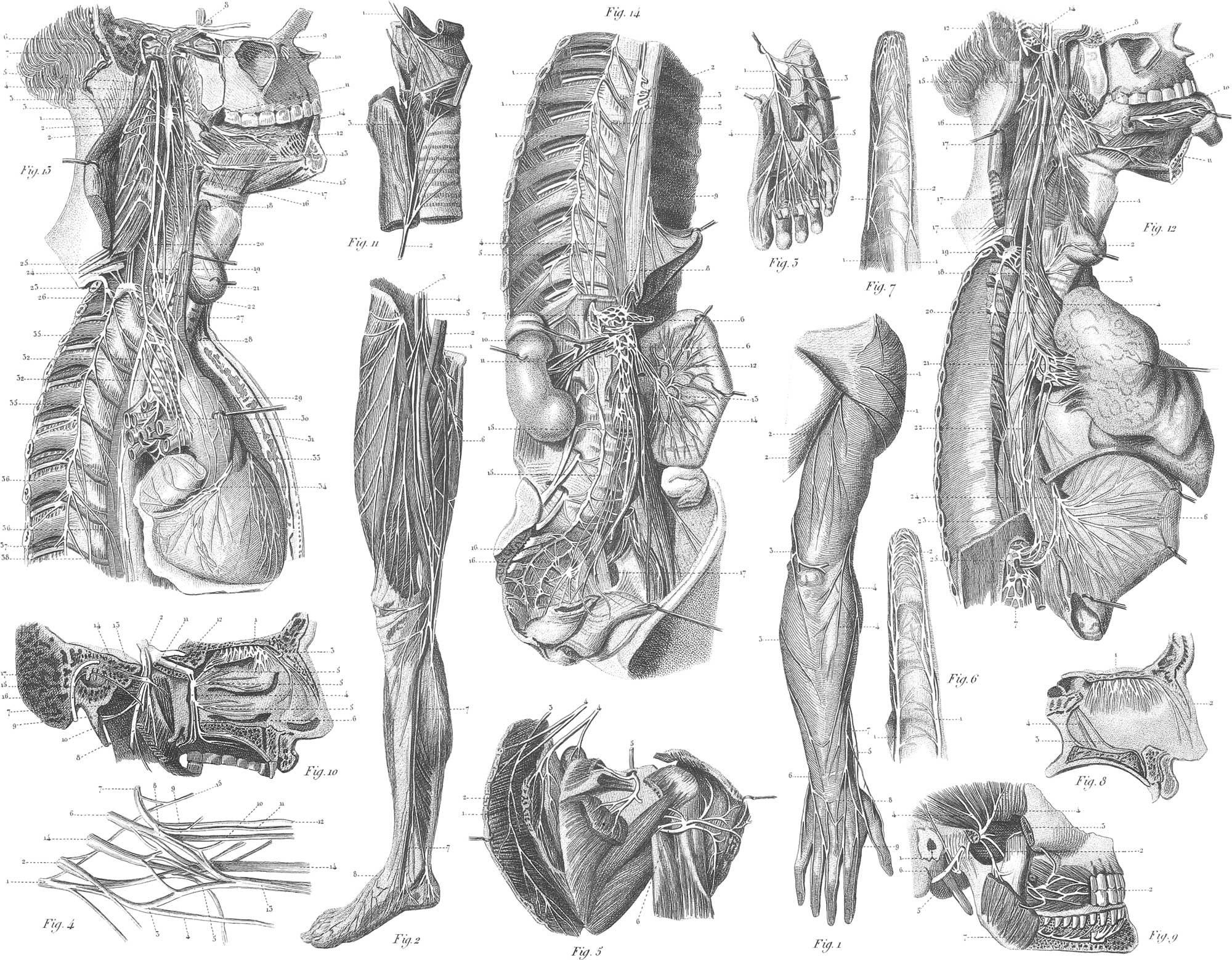
Cerebral Nerves
1. Olfactory Nerves. First Pair. This pair of nerves is the first given off, arising from the inferior anterior surface of the brain. From the bulb which each of these nerves forms at the side of the crista galli, several branches descend into the nose through the foramina in the cribriform plate; they may be divided into the internal, middle, and external. The internal branches, about ten in number, descend in grooves along the septum, and subdivide into many filaments, which form a plexus with each other in the mucous membrane. The middle branches are distributed to the mucous membrane lining the roof of each nostril. The external branches descend along the groove, on the turbinated bones, dividing and communicating frequently with each other, so as to form numerous plexuses which are lost in the pituitary membrane.
2. Optic Nerves. Second Pair. This arises by a broad flattened root, one portion of which comes from the thalamus opticus, and another from the testis; advancing it adheres so closely to its fellow, that the two seem fused together, in such a way that there is no line of separation between them. This junction presents the form of the letter X, and is called the chiasm a. Separating again after this union, each nerve passes through its optic foramen, and piercing the sclerotic and choroid membranes of the eye, expands to form the retina. This nerve is accompanied by the ophthalmic artery. The other nerves distributed to the eye are, the third nerve, the fourth, the ophthalmic branch of the fifth, and the sixth.
3. The Motores Oculi. Third Pair. This arises from the internal face of the crus cerebri, in advance of the anterior margin of the tuber annulare. After passing through the foramen lacerum orbitale, it divides into two branches, a superior and an inferior. The superior or smaller passing above the optic and nasal nerves, divides into two branches, one to the superior rectus, the other to the levator palpebræ. The inferior or the larger branch passes below and to the outside of the optic nerve, and divides into three branches: an internal, to the internal rectus; a middle, to the inferior rectus; and an external, to the inferior oblique.
4. The Trochleator Patheticus. Fourth Pair. This is the smallest nerve coming from the encephalon, not exceeding a sewing thread in thickness. It arises by two roots from the upper anterior face of the valve of the brain, just below the testes; passing through the foramen lacerum orbitale, it reaches the eye, and is distributed to the superior oblique muscle.
5. The Trigemini: Trifacial. Fifth Pair. This emerges by three roots from the side of the pons Varolii, just where it is continuous with the crus cerebelli, and after forming the semilunar or Gasserian ganglion, is divided into three large branches, the ophthalmic, the superior, and the inferior maxillary.
The ophthalmic passes along the outer side of the cavernous sinus, and approaching the foramen lacerum orbitale, divides into three branches, the lachrymal, the frontal, and the nasal. The lachrymal is ultimately distributed to the conjunctiva and lachrymal gland. The frontal divides into an internal or supra-trochleator nerve, to the region of the eye, and the external, supra-orbital, or proper frontal nerve, to the scalp. Both the frontal and lachrymal are nerves of sensation. The nasal nerve divides into two branches, the external or infra-trochleator to the lachrymal passages and the region of the nose, and the internal or proper nasal.
The superior maxillary nerve is larger than the ophthalmic, and passes from the middle of the ganglion forwards through the foramen rotundum into the pterygo-maxillary fossa. Here it sends down two small branches, which ultimately unite in the spheno-palatine ganglion or the ganglion of Meckel. From this proceed three sets of branches, an inferior, internal, and posterior. The inferior or palatine nerves are distributed to the palate and uvula. The internal branch, or the spheno-palatine nerve, divides into several branches after passing into the upper and back part of the nose; the principal of these is the naso-palatine nerve or nerve of Cotunnius. The third or posterior branch of the ganglion is the vidian or superior petrosal nerve, distributed to the tympanic apparatus.
Other branches sent off by the superior maxillary are, the orbital, the malar, the temporal, the posterior dental, the infra-orbital, and the anterior dental, all of which indicate their distribution in their names.
The inferior maxillary nerve descends from the ganglion through the foramen ovale into the zygomatic fossa, where it divides into two large branches, a superior or external, and an inferior or internal. The former subdivides into the two deep temporal, the masseteric, the buccal and the pterygoid; the latter into the auricular, inferior dental, and gustatory nerves; most of these have various subdivisions.
6. Motor Externus Oculi. Sixth Pair. This arises from the base or upper portion of the corpus pyramidale, under the posterior margin of the tuber annulare, or pons; the fibres are assembled into two roots, of which the external is much the larger. These roots, uniting, pass through the sphenoidal foramen, and are distributed to the abductor oculi muscles.
7 a. Facial Nerve or Portio Dura of the Seventh Pair. This arises by two branches; the larger from the medulla oblongata, at the most superior part of the corpus restiforme; the smaller from that portion of the medulla oblongata placed between the first branch and the auditory nerve. The two branches are kept distinct for the distance of several lines, when they unite, and, passing into the meatus auditorius internus and through the aqueduct of Fallopius, emerge at the stylo-mastoid foramen, to be distributed upon the muscles and skin of the head. In the aqueduct of Fallopius it sends off the tympanic branch, and lower down the chorda tympani. Escaping through the stylo-mastoid foramen, it gives off three branches, the posterior auricular, stylo-hyoid, and submastoid or digastric. Further branches and subdivisions are the temporo-facial, with its fasciculi, the temporal, malar, and buccal; and the cervico-facial, still further separated into maxillary, submaxillary, and cervical branches. The portio dura nerve has been supposed to be the exclusive motor nerve of all the superficial muscles of the face, of the eyelids, nose, mouth, lips, and of the ears.
7 b. The Auditory Nerve, or Portio Mollis of the Seventh Pair. This, which is a single nerve of sense, arises partly from the medullary striæ, or the surface of the calamus scriptorius, and partly from the corpus restiforme, between the glosso-pharyngeal nerve and the tuber annulare; it is distributed to the labyrinth of the ear.
8 a. Glosso-Pharyngeal, or First Branch of the Eighth Pair. This arises from the posterior cord of the medulla oblongata, just above and anterior to the superior filaments of the next nerve. Its filaments, therefore, spring from the anterior margin of the corpus restiforme, or from the fissure separating it from the corpus olivare. After the union of its filaments into a round cord, it passes through the foramen lacerum postering, and is ultimately distributed to the tongue and pharynx.
8 b. The Pneumogastric Nerve, or Vagus of the Eighth Pair. This arises from the corpus restiforme of the medulla oblongata, posterior to the highest root of the accessory nerve. It passes through the foramen lacerum posterius, in a canal in common with the spinal accessory, and is separated posteriorly from the internal jugular vein by a small spine of bone. In the foramen it presents a ganglionic expansion, and below it a gangliform swelling, nearly an inch in length; the latter communicates beneath the base of the cranium, and in front of the two first cervical vertebræ, with the facial, glosso-pharyngeal, spinal accessory, sympathetic, and superior spinal nerves, constituting the basilar plexus. Descending towards these organs, it gives off cervical, thoracic, and abdominal branches. The cervical branches are the communicating, the auricular, the pharyngeal, the superior laryngeal, the cardiac, and the recurrent or inferior laryngeal. The thoracic gives off the pulmonary and the œsophageal nerves, the former presenting the anterior and posterior pulmonic plexus, the latter the œsophageal plexus. On the right stomach, the right vagus passes behind the cardiac orifice; and its branches, with some others, unite to form the cardiac plexus. The pneumogastric nerves supply the pharynx, œsophagus, and, partly the stomach; also the larynx, trachea, lungs, and partly the heart; they are, therefore, concerned in deglutition, voice, respiration, circulation, and digestion, and maintain important sympathies between the different organs concerned in these functions.
8 c. The Nervus Accessorius, or Spinal Accessory. This is the third branch of the eighth pair. It arises from the posterior fasciculus of the medulla oblongata, just above the hypoglossus nerve, and also from the posterior fasciculus of the medulla spinalis; with a variable number of roots, it passes through the foramen lacerum posterius, to be distributed to the muscles and integuments of the neck. This nerve is supposed to be compound, but essentially motor, and has been termed “the respiratory nerve of the neck.”
9. The Lingual Nerve; Hypoglossal Nerve. Ninth Pair. This arises from the medulla oblongata, by several fasciculi, whose roots spring from the fissure which separates the corpus pyramidale from the corpus olivare; these unite into two or three trunks, which ultimately coalesce into one which passes through the anterior condyloid foramen of the occipital bone, to be distributed to the muscles of the tongue. As it passes across the neck, below the digastric tendon, it gives off a considerable branch, the descendens colli or noni, to the omo-hyoid, sterno-hyoid, and thyroid muscles.
Pl. 137, fig. 17, branches of the fifth pair: 5, infraorbital; 6, frontal; 7, lachrymal; 8, buccal; 9, superficial temporal; 10, mental; 11, hypoglossus; 12, trunk of the facial nerve, exterior to the aqueduct of Fallopius. For the distribution of the facial nerve see fig. 18, near the third branch of the fifth pair. Fig. 18 1, stem of the fifth pair; 2, spheno-palatine ganglion; 3, superficial branch of the vidian nerve, its connexion with the sympathetic in the foramen lacerum, and with the facial nerve; 4, lingual branch of the fifth pair, and the union of the chorda tympani with it; 5, ganglion oticum, with its branches; 6, facial nerve; 7, union of the vidian nerve with the facial; 8, origin of the chorda tympani from the facial nerve; 9, union of the facial nerve with the glosso-pharyngeal; 10, with the vagus; 11, glosso-pharyngeal nerve with the ganglion petrosum, from which proceeds the plexus of Jacobson; 12, carotid plexus. Fig. 19, ophthalmic branch of the fifth pair: 1, skin of the forehead reflected; 2, optic nerve; 3, oculo-motor nerve; 4, sixth pair; 5, ophthalmic branch of the fifth pair; 6, lachrymal nerve; 7, its anastomoses with the fourth pair; 10, ethmoid nerve. Fig. 20, superior maxillary branch of the fifth pair: 2, lachrymal nerve; 2, second branch of the fifth pair; 3, spheno-palatine ganglion; 4, superficial branch of the vidian nerve; 5, deeper branch; 6, posterior dental nerve; 7, branch to the gums; 8, anterior dental nerve; 9, dental plexus; 10, infra-orbital nerve; 11, masseteric nerve; 12, superficial temporal; 13, inferior maxillary nerve, cut off; 14, lingual nerve, with its connexion with the chorda tympani; 14′ (beneath 16), submaxillary ganglion; 15, glosso-pharyngeal; 15′, accessory of Willis; 16, vagus; 17, hypoglossus nerve, or ninth pair; 18, internal carotid artery. Fig. 21 1, inferior maxillary, within the foramen rotundum; 2, temporal nerve; 5, masseteric nerve; 6, superficial temporal nerve, and its connexion with the facial; 7, inferior dental; 8, mental; 9, lingual, with the chorda tympani: 10, internal pterygoid.
Pl. 138, fig. 9, inferior maxillary branch of the fifth pair, from outside: 1, masseteric; 2, buccal; 2′, its ramifications on the outside of the buccinator muscle; 3, external pterygoid; 4, 4, deep temporal nerves; 5, superficial temporal; 6, facial nerve; 7, dental nerve of the lower jaw. Fig. 10, fifth pair, from within: 1, distribution of the nerve of smell on the spongy bones; 2, trigemini nerve, Casserian ganglion, and origin of the three principal branches; 3, external or lateral nasal branch; 4, spheno-palatine ganglion; 5, 5, 5, posterior nasal nerves; 6, palatine nerves; 7, lingual nerve and chorda tympani; 8, submaxillary nerve; 9, superficial temporal nerve; 10, inner pterygoid; 11, ganglion oticum; 12, threads from it to the tympanum, and to the mucous membrane of the nose; 13, connecting branch to the facial nerves; 14, threads to the tensor tympani; 15, threads to the plexus, along the internal maxillary artery; 16, facial nerve; 17, chorda tympani.
Pl. 138, fig. 11, nerves of the larynx: 1, superior, 2, inferior laryngeal nerves; 3, union of the two. Fig. 12 1, laryngeal; 2, thyroid gland; 3, trachea; 4 arteria innominata; 5, right lung; 6, stomach; 7, great cœliac plexus; 8, 9, glosso-pharyngeal nerve; 10, lingual branch of the fifth pair; 11, hypoglossus; 12, accessory nerve; 13, division into the muscular branch and into the branch to the tenth pair; 14, vagus; 15, its pharyngeal branch uniting with threads of the glosso-pharyngeus and sympathetic us to form the pharyngeal plexus; 16, superior laryngeal nerve and its division into an outer and an inner branch; 17, 17, 17, nerves of the heart; 18, off-shoot of the recurrens; 19, inferior cervical plexus of the sympatheticus; 20, tracheal branch; 21, pulmonic plexus; 22, pharyngeal nerves; 23, entrance of the right vagus into the cœliac plexus; 24, left trunk, and its distribution on the stomach; 25, cœliac plexus.
Spinal Nerves
There are thirty-one pairs of spinal nerves, each arising by two roots, an anterior or motor root, and a posterior or sensitive root.
The anterior roots proceed from a narrow white line, anterior lateral sulcus, on the antero-lateral column of the spinal cord, and gradually approach towards the anterior longitudinal fissare as they ascend. The posterior roots proceed from the posterior lateral sulcus, a narrow grey stria, formed by the internal grey substance of the cord.
After the formation of a ganglion the two roots unite and constitute a spinal nerve. The spinal nerves are divided into cervical, dorsal, lumbar, and sacral. The cervical nerves pass off transversely from the spinal cord; the dorsal are oblique in their direction, and the lumbar and sacral vertical; the latter form the large assemblage of nerves at the termination of the cord called cauda equina.
1. The Cervical Nerves are eight in number, increasing in size as they descend; the first passes out above the atlas, and is named the sub-occipital; the eighth passes out above the first dorsal vertebra. All of these, except the first and second, immediately outside the intervertebral foramina, divide into a posterior and an anterior branch; the posterior of each is generally the smaller. The anterior branches of the first four form the cervical plexus, and those of the last four with the first dorsal, the brachial plexus.
2. The Cervical Plexus is formed by the loops and communications between the anterior branches of the four superior cervical nerves, which join each other in arches, from the convexities of which branches arise that again join in a similar manner: lymphatic glands and a quantity of cellular tissue are entangled in the areolæ between these. This plexus communicates with the superior cervical ganglion of the sympathetic above, and with the continued cord of this nerve lower down; also with the pneumogastric, lingual, and spinal accessory. Besides numerous muscular filaments, it sends off various cutaneous branches, which are either ascending or descending.
The ascending branches are: a. Superficialis colli, arising about the middle of the neck, and distributed on the anterior and lateral region of the neck. b. The auriculciris magnus arises in the same situation and ascends nearly parallel and posterior to it; at the parotid gland it divides into two branches, one superficial, the other deep, which supply the external ear and sides of the scalp, c. The occipitalis minor arises near the last from the second cervical nerve, and ascending is distributed to the skin and occipito-frontalis muscle.
The descending branches are superficial and deep. The superficial branches, or supra-clavicular, are long and rather large; they arise from the third and fourth cervical nerves, and pass to muscles of the neck and shoulder. The deep descending branches are: a. The muscular. These arise from different parts of the plexus, and are principally distributed to the trapezius, levator anguli scapularis, and sterno-mastoid muscles, b. The communicating branches are very numerous. From the second and third roots of the plexus descends the communicans noni to the hyoid apparatus c. The most important branch of the cervical plexus is the internal respiratory or phrenic nerve. This arises from the lower part of the plexus, and descending on the anterior scalenus muscle, enters the thorax between the subclavian vein and artery; passing down the middle mediastinum to the diaphragm on the side of the pericardium, the left phrenic takes an oblique course round the base of the heart.
Pl. 137, fig. 15, superficial nerves of the cervical plexus: 1, superficial temporal nerve of the fifth pair; 2, occipitalis magnus; 3, superior cutaneous cervical nerve, from the facial; 4, auricularis magnus; 5, occipitalis minor; 6, an inconstant occipital nerve, 7, 7, some posterior cutaneous branches; 8, accessory nerve; 9, supra-scapular nerve; 10, supra-clavicular nerve; 11, middle cutaneous cervical nerve; 12, a small branch accompanying the jugular vein; 13, connexion of the cervical plexus with the facial nerve.
The anterior divisions of the last four cervical, and that of the first dorsal, unite to form the brachial plexus.
3. The Brachial Plexus. This plexus is broad and flat, the nerves forming it being very large, particularly the inferior. It is situated at the lower and lateral parts of the neck, between the scalenic muscles and the subclavian artery; it then passes under the clavicle into the axilla, where it rests on the serratus magnus, ending opposite to the coracoid process. The numerous branches of this plexus may be arranged into two orders, one (supra-clavicular) arising above the clavicle, the other (axillary) arising from below this bone.
The supra-clavicular branches are as follows: 1. For the subclavian muscle. 2. Small branches from the upper root of the plexus to the scaleni, levator anguli, and rhomboidei muscles. 3. Posterior thoracic or external respiratory, from the fifth and sixth cervical. It descends obliquely outwards behind the brachial plexus, and passing along the serratus magiius, supplies it with fasciculi. 4. The supra-scapular form the upper division of the plexus. Descending it gives off branches to the supra-spinatus, infra-spinatus, teres minor, and to the shoulder-joint.
The infra-clavicular, or axillary branches, are the thoracic, the sub-scapular, and the circumflex, to the pectoral muscles, the axilla, and the shoulder; the internal cutaneous, external or musculo-cutaneous, median or brachial, and the ulnar, to the anterior and internal aspect of the arm, forearm, hand, and fingers; the musculo-spiral, or radial nerve, to the supinators of the forearm, hand, and fingers. Some of these branches we shall now notice more in detail.
The median or brachial nerve is the largest branch of the plexus; it generally arises by two roots, one in common with the external cutaneous, from the upper part of the plexus, the other internal, from the lower end of the plexus in common with the ulnar and internal cutaneous. The brachial artery usually separates these two roots, which soon unite into one thick cord, passing down superficially as far as the bend of the elbow; at the end of the elbow it passes along the brachialis anticus, and perforating the pronator, descends along the middle of the forearm, and terminates in the hand by five or six branches. A little below the elbow this nerve gives off the anterior interosseal nerve.
The ulnar nerve arises from the lower part of the plexus in common with the internal cutaneous and the inner head of the median; descending the arm, it passes behind the elbow-joint through the groove between the inner condyle and the olecranon process; it then passes forwards and descends along the ulnar side of the forearm to the carpus, and passing over the annular ligament close to the pisiform bone, ends in the palm of the hand in two branches, a superficial and a deep. A little above the wrist it gives off the dorsalis carpi ulnaris, a large branch which winds round the ulna to the back of the hand, there dividing into several long branches.
Connected to the digital and other sensitive branches both of the median and ulnar nerves are a number of small indurated white bodies, now known by the name of Pacinian corpuscles from their discoverer. They appear like globules of firm cellular membrane, in size from \(\frac{1}{20}\) of an inch upwards, and connected to the nerve by a short delicate nervous stem. The corpuscle itself is found to consist of a great number of concentric membranous capsules, with intervening clear fluid. Their function is unknown. Pacini suggested that they might in some way be connected with the phenomena of animal magnetism; others see in them an analogy to the electrical organ of fishes. They are especially abundant in the mesentery and mesocolon of the cat. Similar sessile bodies have recently been discovered by Leidy in the intercostal nerves of the boa constrictor.
The muscido-spiral or radial nerve is the largest branch in the plexus; it proceeds from the middle and lower divisions in common with the circumflex nerve, and descending to the elbow there divides into two branches, an anterior or radial branch and a posterior or interosseal branch, previously to which it sends off various muscular and cutaneous branches. The anterior or radial nerve supplies the supinator longus muscle, along which it descends, and passing behind its tendon about the middle of the forearm, becomes cutaneous; continuing in its decent, it divides into two considerable branches on the back of the head. The deep branch, or the posterior interosseal nerve, is larger than the radical; winding around the upper part of the radius, it descends along the back part of the forearm, and divides into several branches, superficial and deep, which supply the two layers of extensor muscles.
Pl. 137, fig. 16 (see fig. 15, for the four superior cervical nerves), deep cervical nerves; brachial plexus: 1, facial nerve; 2, vagus; 3, internal carotid artery; 4, accessory nerve; 5, its connexion with the cervical nerves; 6, hypoglossus; 7, anterior branch of the first cervical nerve, uniting with the hypoglossus and vagus; 8, connecting branches of the second and third cervical nerves with the hypoglossus; 9, phrenic nerve; 10, 10, deep branches of the cervical plexus; 11, brachial plexus; 12, the nerve for the subclavian muscle giving off a branch to the phrenic nerve; 13, anterior thoracic nerve; 14, posterior do.; 15, 16, 17, branches of the subscapular nerve, to the subscapularis, the latissimus dorsi, and teres muscles; 18, axillary artery, embraced by the brachial plexus; 19, brachial branches of the brachial plexus.
Pl. 138, fig. 1, cutaneous nerves of the arm, on the dorsal side: 1, cutaneous branches from the axillary nerve; 2, 2, from the radial nerve; 3, 3, branches of the internal cutaneous; 4, 4, branches of the external cutaneous; 5, union of one of these branches with the radial nerve; 6, dorsal branch of the ulnar nerve with its digital branches; 7, dorsal branch of the radial nerve and its digital branches; 8, connecting branches between the radial and ulnar nerves; 9 bifurcation of a digital nerve. Fig. 5, 1, trapezius muscle; 2, rhomboideus do.; 3, accessory nerve; 4, 4, deep posterior branches from the cervical and brachial plexus: 5, supra-scapula nerve; 6, axillary nerve or circumflex nerve of the arm.
The share of the brachial plexus possessed by each nerve of the superior extremities in the brachial plexus may be expressed as follows, the figures referring to the 5th, 6th, 7th, and 8th cervical nerves, and to the 1st dorsal nerves, which together constitute this plexus.
- The supra-scapular nerve, 5, 6, or 5, 6, 7.
- The subscapular nerve, 5, 6, 7, 8, or 5, 6, 7.
- The anterior thoracic, 5, 6; the posterior often 8, 1.
- The great internal cutaneous nerve of the a,rm, 8, 1, or 7, 8, 1, or 1.
- The musculo-cutaneous nerve, 5, 6, 7, or 5, 6, or 5, 7.
- The axilliary nerve, 5, 6, 7, or 5, 6, or 5, 6, 7, 8, 1.
- The radial nerve, 5, 6, 7, 8, or 5, 6, 7, 8, 1, or 6, 7, 8, or 6, 7, 8, 1, or 5, 6, 7, or 7, 8.
- The ulnar nerve, 5, 6, 7, 8, 1 or 5, 6, 7, 8, or 6, 7, 8, 1, or 6, 7, 8, or 7, 8, 1, or 8, 1.
- The median nerve, 5, 6, 7, 8, 1, or 5, 6, 7, 8, or 5, 7, 8, 1, or 6, 7, 8, 1, or 5, 6, 7, 1, or 8, 1.
- The posterior thoracic, 5, 6, 7, 1.
Pl. 138, fig. 4, brachial plexus unravelled: 1, 2, fifth and sixth cervical nerves; 3, branch arising from the union of the two and dividing into 4, the musculo-cutaneous nerve, and 5, a connecting branch of the median nerve; 6, 7, eighth cervical and first dorsal nerve; 8, their connexion, and 9, their division into a branch going to the median nerve, the ulnar nerve 10, and the internal cutaneous nerve 11; 12, small internal cutaneous nerve; 13, median nerve; 14, 14, radial nerve; 15, posterior thoracic. Fig. 6, relations of the digital nerves or the palmar side: 1, 1, digital nerves; 2, plexus at the tip of the finger formed by the union of the two. Fig. 7, relations of the digital nerves or the dorsal surface: 1, 1, dorsal nerves; 2, 2, branch of the preceding nerves passing round to the dorsal surface.
4. The Dorsal Nerves are twelve in number on each side. The first pair passes between the two first dorsal vertebræ, the last pair between the last dorsal and first lumbar vertebræ; the first is very large, the following diminish in size, but the two last again increase, and the twelfth is nearly equal to the first. These nerves are distributed to the parietes of the thorax and abdomen, also to the muscles and integuments on the posterior and lateral regions of the trunk; they are not connected together in any plexus like the cervical, lumbar, and sacral nerves, but are distributed separately. All their anterior branches, however, are united through the medium of the chain of the dorsal sympathetic ganglions, each of the former being connected by one or two filaments to one of the latter; the first dorsal also joins to the last cervical in the brachial plexus, and the last dorsal is connected to the first lumbar; they all divide into a posterior and an anterior or intercostal branch. The posterior or dorsal branches are smaller than the anterior; they each pass backwards, accompanied by the posterior branch of the intercostal artery, through a foramen formed above and below by the spinous processes, internally by the bodies of two vertebræ, and externally by the anterior or great costo-transverse ligament; they supply the muscles and integuments of the back and loins.
The anterior dorsal nerves, excepting the first, are named the intercostals, and pass round the parietes of the thorax between the laminæ of the intercostal muscles, and inferior to the intercostal blood-vessels: the superior five or six are confined to the chest, and extend as far as the sternum; the anterior portions of the inferior five or six are placed in parallel lines between the abdominal muscles, and extend to the rectus. They supply the parietes, muscles, and integuments of the thorax and of the upper part of the abdomen.
5. The Lumbar Nerves. There are five pairs. They are larger than the dorsal, and increase in size downwards; the first escapes between the two first lumbar vertebræ, the fifth between the last vertebræ and the sacrum; like the dorsal, they divide into posterior and anterior branches. The posterior pass between the transverse processes to the lumbo-spinal muscles, and each divides close to the multifidus spinæ into an internal and external branch; the former is lost in the multifidus spinæ, inter-spinous, and inter-transverse muscles; the external branch is large and musculocutaneous, supplying the sacro-lumbalis and lumbar aponeurosis. The two last posterior nerves are very small, and are distributed to the integuments of the guteal region.
The anterior branches of the lumbar nerves are much larger than the posterior, and increase in size as they descend. In the psoas magnus muscle they unite with each other into a plexus.
6. The Lumbar Plexus is long and somewhat triangular, situated along the sides of the lumbar vertebræ, in front of their transverse processes, and near the posterior surface of the psoas magnus muscle; in addition to its three principal and terminal branches, the anterior crural, the obturator, and the lumbo-sacral, it gives off some long superficial branches.
The superficial hranches of the lumbar plexus supply the inferior portion of the abdominal muscles and integuments, the integuments of the groin, of the upper and outer part of the thigh, and also those of the inguinal and pubic regions. The principal of these are the superior musculo-cutaneous (external ilio-inguinal, ilio-hypogastric, ilio-scrotal), the middle musculo- or inguino-cutaneous, the inferior musculo-cutaneous or external cutaneous, and the genito-crural.
The anterior crural nerve arises in the lumbar plexus from the four superior nerves, principally from the third and fourth; it is destined to supply the integuments on the anterior and inner sides of the lower extremities, also extensors of the leg, and the principal flexors of the thigh or hip-joint. It subdivides into a superficial and a deep fasciculus. The principal branches of the superficial division are, the middle cutaneous, the internal cutaneous, the vaginal branches to the sheaths of the vessels, and the long saphena. The branches of the deep division are wholly muscular.
The obturator nerve arises chiefly from the third and fourth lumbar, perforates the psoas muscle, and descends obliquely inwards to the inside of the thigh, where it descends into two branches, an anterior and a posterior. The anterior or superficial branches are lost in the graciles, adductor brevis, pectinæus, and vastus externus. The posterior or deep branches supply the obturator externus and adductor magnus; one long branch extends to the back part of the knee joint.
The lumbo-sacral nerve is the largest branch of the lumbar plexus; it is formed by a large portion of the anterior division of the fourth, and the whole of that of the fifth lumbar nerves; enters the pelvis, and behind the iliac vessels divides into two branches. Of these, the communicating is inferior or anterior, and joins the first anterior sacral nerve, forming part of the sacral plexus; the other, posterior and superior, is the great or superior glutæal nerve. This has various muscular branches for the muscles of the thigh.
7. The Sacral Nerves are six pairs. They form their ganglions, and divide within the spinal cord into anterior and posterior branches. The posterior sacral nerves are very small, pass through the posterior sacral foramen, and supply the muscles and integuments of the sacral and glutæal regions.
The anterior social nerves are very large, especially the three superior; the three last are much smaller, and the sixth is very minute, and sometimes wanting. The four superior, with the branch from the last lumbar, form the sacral plexus, placed on the sacrum behind the pelvic fascial; its form is somewhat triangular or palmate. Each of the sacral nerves, immediately after its emergence from the foramen, is joined by a short branch from one of the ganglions of the sympathetic. The sacral plexus sends off the following branches, both internally and externally: the internal or pelvic are the hæmorrhoidal, vesical, and muscular, and in the female the uterine and the vaginal; the external branches are the inferior or lesser sciatic, the inferior glutæal, posterior cutaneous, pudic, and great sciatic or posterior crural. All these escape by the lower part of the great sciatic notch below the pyriform muscle. The visceral branches arise from the fourth and fifth sacral, and are directed forwards into the cavity, there to be joined by numerous filaments from the sympathetic nerve, forming the hypogastric plexus, a complex network of nervous filaments entangled around the branches of the internal iliac artery, and accompanying them to their terminations.
The internal or pelvic muscular branches supply the levator ani, obturator internus, pyriformis, and sphincter ani. The lesser sciatic, inferior glutæal, and posterior cutaneous nerves, may all be regarded as one large, loose, and flat fasciculus, escaping from the pelvis below the pyriform muscle; branches are distributed to the perinæal regions, and to the upper part of the leg.
The pubic nerve arises from the third and fourth sacral, and, passing through the great sciatic notch or foramen, re-enters the pelvis by the lesser sciatic notch, and proceeds towards the pubes; it then divides into two branches, an inferior and a posterior. The inferior or perinæal nerve, the larger of the two, is distributed to the muscles and integuments of the perinæum. The superior branch continues along the pubes to the symphyis, and is finally distributed to the subcutaneous cellular tissue of the glans penis.
The great sciatic, or posterior crural nerve, is the principal branch of the sacral plexus, and the largest nerve in the body. It proceeds from the four superior sacral nerves, forms a flat broad band, which escapes from the pelvis below the pyriform muscle, and descends close to the outer side of the tuber ischii, along the back part of the thigh, as far as the ham, where it divides into the external and internal poplitæal nerves, having given off numerous muscular and cutaneous branches. About the middle of the thigh it often gives off a large nerve, the external articular, to the outer side of the knee joint.
The external poplitæal, or the peronæal nerve, is destined to supply the muscles on the external and anterior aspect of the leg, as also the integuments of the leg and dorsum of the foot. Descending, it gives off several long branches, termed the external cutaneous nerves of the leg; one of these, the communicans peronæi, passes backwards over the outer part of the gastrocnemius, and communicates with the external saphenous nerve. Passing round the joint of the fibula, the peronseal nerve divides into two branches, the musculo-cutaneous and the anterior tibial. The musculo-cutaneous passes down the leg, and a little above the external malleolus, divides into the internal and external tarsal nerves, or the dorsal nerves of the foot. The anterior tibial, or interosseal nerve, supplies muscles of the leg, and on the tarsus divides into an external and internal branch, the latter of which, the continued trunk, passes to the first and second toes.
The internal poplitæal or posterior tibial nerve, is much larger than the preceding, being destined to supply the large muscles on the back of the leg, and the muscles and integuments of the sole of the foot. In the ham it gives off various articular branches, and one principal cutaneous branch, the external saphenous. Continued down the leg, the posterior tibial nerve, at the tendo Achillis, gives off several large branches, as the external and internal plantar to the lower surface of the foot.
Pl. 138, fig. 2, crural nerve, and its distribution: 1, crural vein; 2, crural artery; 3, crural nerve; 4, external cutaneous nerve; 5, branches embracing the vessels; 6, saphena; 7, 7, saphenous nerve; 8, cutaneous branch from the peronseal nerve to the foot. Fig. 3, nerves of the sole of the foot: 1 division of the posterior tibial nerve into 2, the inner, and 3, the outer plantar nerve; 4, division of the inner plantar nerve into four digital nerves; 5, division of the outer into a superficial and a deep branch.
Sympathetic System
In addition to the five small ganglions on each side, already noticed in the description of the cerebral nerves, viz. the Casserian, the lenticular or ophthalmic, the spheno-palatine or Meckel’s, the sub-maxillary, the otic or the ganglion of Arnold: also, the several ganglions on the posterior roots of the spinal nerves: we find one continued chain of these bodies placed along the vertebral column, on either side of the median line, and at regular intervals. These ganglions, on each side, are all connected to each other, and resemble a knotted cord; these cords receive the name of the sympathetic nerves.
The sympathetic nerves, therefore, are two in number: they descend from the base of the cranium perpendicularly along the neck, and are placed anterior to the vertebra, on the rectus capitis and longus colli muscles, and behind the great vessels and nerves. At the upper end of the chest, each of these nerves is divided by the subclavian artery into several branches, which encircle that vessel, and unite below it in the thorax. Through this cavity they descend, at first obliquely, backwards, and outwards, along the side of the spine, over the heads of the ribs and their stellate ligaments, and are covered by the pleura; they then incline a little forwards, and pass behind the true ligamentum arcuatum into the abdomen; through this region they descend obliquely outwards on the fore part of the lumbar vertebræ, between the psoas muscles and the crura of the diaphragm; they then sink into the pelvis, keeping close to the sacrum, and descend along the anterior surface of this bone obliquely inwards; near its inferior extremity, or on the first part of the coccyx, they unite and terminate in a small ganglion, named coccygeal, or impar. The superior extremity of each sympathetic nerve is connected by several filaments with several of the cerebral nerves. Some of these connexions, particularly that with the sixth, have been improperly termed the origin of the sympathetic; at the base of the cranium it communicates, either directly or indirectly, with the seventh, eighth, and ninth; in the cavernous sinus and orbital plexus with the third, fourth, fifth, and sixth; and even with the olfactory, optic, and auditory, by the fine filaments which accompany the nutrient arteries of those several organs in which these nerves expand and terminate; it also communicates, as has been already noticed, with the several ganglions in the head. In their course along the spinal column, each nerve regularly communicates with every pair of the spinal nerves, with each of the carvical nerves by one and sometimes by two filaments, and with each of the dorsal, lumbar, and sacral nerves by two, so that these nerves may be said to communicate with every nerve in the cerebro-spinal system. The sympathetic nerves have been considered by some as independent nervous systems, communicating by numerous branches with every portion of the cerebro-spinal system; by others they are regarded as nervous cords, formed by the union of branches from all the spinal and from several of the cerebral nerves: the latter is probably the more correct view.
Although perfect symmetry does not exist between these nerves on the right and left sides, yet the differences are but trifling. The sympathetic nerves send off numerous branches, which are chiefly destined to supply the heart and the coats of the great vessels, and all the pelvic and abdominal viscera, except the stomach. These branches arise from the ganglions on these nerves; of these there are generally three in the neck; in the back and loins they correspond with the number of vertebræ in those regions, and in the pelvis there are three on each side, and the coccygeal or impar ganglion below.
The cervical ganglions are three, the superior, middle, and inferior. Sometimes, however, there are four, and at others only two.
The superior cervical ganglion is of an oval figure and reddish color, extending from the first to the third cervical vertebra; its upper end is very small, and about half an inch beneath the carotid foramen in the petrous bone. It sends off several branches, superior, inferior, internal, external, and anterior. The superior branches are two in number; they ascend in the carotid canal to the cavernous sinus, and communicate with the sixth and the vidian branch of the fifth. In the carotid canal they form the internal carotid plexus, from which some filaments pass through the petrous bone into the tympanum. In this sinus, the ascending small filaments again form a plexus named cavernous plexus. From this plexus, filaments pass to the Casserian ganglion, others to the orbital plexus and lenticular ganglion, and the remainder accompany the artery to the brain. The inferior or descending branch is the continued cord of the sympathetic itself which joins the middle or cervical ganglion. The anterior branches are numerous; some communicate with the eighth and ninth in the great basilar plexus, others surround the external carotid, and divide into fasciculi which accompany all its branches and form loops and plexuses around each, named from their destination, thyroid, lingual, &c. The external branches join the superior cervical nerve; they are large and ganglionic. Some join the nervous loop, the principal unite with the second cervical and others with the third and fourth. The internal branches are pharyngeal, laryngeal, and cardiac. The pharyngeal arise from the superior part of the ganglion; are of a pale red color and ganglionic structure; they pass inwards and join the pharyngeal branches of the glosso-pharyngeal and pneumogastric in the extensive plexus which supplies the pharynx and fauces. The laryngeal branches arise near the last, pass downwards and inwards, and join the branches of the superior laryngeal nerve. The superior cardiac, or superficialis cordis, arises near the lower part of the ganglion, and descending, enters the chest, and joins the great cardiac ganglion.
The middle cervical ganglion, smaller than the superior, is sometimes wanting. It is situated behind the carotid opposite to the fifth vertebra; from its anterior aspect it sends off the middle or great cardiac nerve, which enters the chest, and with the superior and inferior cardiac nerves joins the cardiac plexus and ganglion.
The inferior cervical ganglion is of an irregular figure, semilunar or triangular, and frequently appears to consist of several small ganglions connected with each other by reddish filaments. It is situated between the transverse process of the last cervical vertebra and the neck of the first rib; filaments from it communicate with the phrenic nerve and with the brachial plexus; its external branches join the three last cervical and first dorsal nerves. From its inferior aspect proceed the inferior cardiac nerves, which communicate with the middle, and with branches form the vagus and recurrens, ending in the cardiac plexus.
Cardiac Nerves, Ganglion, and Plexus, The superior cardiac nerve arises from the inner part of the superior cervical ganglion, and descends to the chest communicating with various nerves, and ultimately joining the cardiac plexus, the recurrens, and other nerves. The middle cardiac nerve arises from the middle cervical ganglion, or from the sympathetic nerve about the middle of the neck; it descends either in a single cord or in several parallel filaments into the thorax, where it is joined by large branches from the vagus and recurrens nerves; continuing its descent it terminates in the cardiac ganglion or plexus. The inferior cardiac nerve or nerves proceed from the inferior cervical ganglion, and terminate either on the fore part of the aortic arch, or in the anterior cardiac plexus.
The cardiac ganglion is situated within the arch of the aorta; it is joined by the right and left superior cardiac nerves, and by branches from the pneumogastric.
The great cardiac plexus is situated behind the ascending aorta, and consists of a plexus of nerves formed by the middle and inferior nerves from opposite sides, also by branches from the eighth pair, and the recurrent nerves. The roots of the large vessels and the structure of the heart are supplied by the branches from the great cardiac ganglion and plexus, and from the cardiac nerves. These branches form two smaller plexuses, the anterior cardiac or coronary, and the posterior plexus.
In the thorax the sympathetic nerves have twelve ganglions on each side of the spine; sometimes but eleven, when the last cervical and first dorsal are united into one. Each of the thoracic ganglions is small, fiat, and triangular, the base towards the spine, the apex external, covered by the pleura and a thin fascia. All communicate by their external branches with the anterior or intercostal branches of the spinal nerves. From the base or anterior edge of each ganglion, arise the internal branches, the mediastinal, and the great and lesser splanchnic.
The great splanchnic nerve arises by four or five distinct roots from the sixth, seventh, eighth, ninth, and tenth ganglions; they descend forwards and unite into a long, flat cord which enters the abdomen, where each nerve expands into the semilunar ganglion. The real origin of this nerve is from the cerebro-spinal system.
The lesser splanchnic nerve arises by two roots from the tenth and eleventh ganglions, which unite on the side of the last dorsal vertebra. The small nerve thus constituted enters the abdomen through the crus of the diaphragm, and then ends in the renal plexus.
The semilunar ganglion of each side is situated on the diaphragm, and partly on the aorta, on either side of the cœliac axis, and above and behind the supra-renal capsule. These are the largest ganglions on the sympathetic; though called semi-lunar, their form is very variable and irregular, and frequently instead of a single mass they consist of a congeries of knotted ganglions on the nervous cord; the right and left communicate with each other by several filaments, on which again small ganglions are placed. This communication surrounds the cœliac axis, and, as branches radiate from it in all directions, it is termed the solar plexus. This plexus is situated in the epigastrium, behind the stomach, in front of the aorta, and above the pancreas. In this plexus there are also some filaments from the lesser splanchnic and phrenic nerves, and the right vagus terminates in it; it is the most highly developed portion of the sympathetics, and has been regarded as the head or centre of the great organic nervous system by some, who maintain the independence of the ganglionic system and its distinctness from the cerebro-spinal nerves. From it numerous nerves pass off in various directions; these nerves accompany the blood-vessels, and form plexuses around each, which are named, according to their destination, hepatic, splanchnic, gastric, &c.
- The phrenic plexuses consist of branches arising on each side from the upper part of the solar plexus, accompany the phrenic arteries, and enter the diaphragm beneath the peritonæum; some branches follow the phrenic vessels, others pass in different directions, and join some minute filaments from the phrenic nerves of the cervical plexus.
- The supra-renal plexuses arise partly from the last, and, by some delicate filaments from the semilunar ganglion of each side, they twine aroundthe arteries which conduct them into the supra-renal bodies.
- The coronary or gastric plexus. This fasciculus arises from the upper and anterior part of the solar and from the right vagus, and accompanies the arteria coronaria ventriculi, along the lesser curvature of the stomach, to the lesser omentum; its filaments are lost in the submucous tissue, and communicate with those of the right and left; vagi.
- The hepatic plexus is a very large fasciculus, arising partly from the solar and partly from the semilunar ganglions; its large posterior filaments accompany the vena porta, and its anterior the hepatic artery; these nerves accompany the vessels in the lesser omentum to the liver: some are very large and distinct; they enter the transverse fissure, and ramify along with the vessels through the capsule of Glisson. While in the lesser omentum, they send long filaments to form the right gastro-epiploic plexus, along the great border of the stomach; others, also, along the cystic artery to the gall bladder.
- The splenic plexus proceeds in a similar manner around the splenic artery; it is not so large as the hepatic; it sends many filaments to the pancreas, to the great end of the stomach, and along the left epiploic artery to its great curvature; the remaining few filaments enter the spleen.
- The superior mesenteric plexus is a very broad and thick fasciculus continued from the lower border of the solar; it forms a complete sheath for the superior mesenteric artery; its branches are numerous, very long, and distinct; they accompany the arteries, but are straight, and do not form the same number of arches as the vessels are remarkable for: near the intestine many of them usually unite in an arch, from which fine filaments enter the tissues of the intestine. This plexus supplies all the small intestines, the cœcum, ascending colon, and right portion of its transverse arch.
- The renal plexuses are formed by branches from each side of the solar, joined by the lesser splanchnic nerves; they surround the renal arteries, and accompany them into the kidneys. In the male, each renal plexus gives off a fasciculus to accompany the spermatic artery, around which it forms the spermatic plexus, and descends to the testis: in its course along the psoas muscle it gives off filaments to the ureter. In the female, corresponding branches from the renal plexuses supply each ovary.
- The inferior mesenteric plexus is much smaller than the superior, from the root of which it is principally derived, being also joined by branches from the lumbar ganglions of the sympathetic: it accompanies the inferior mesenteric artery and its branches, and supplies the left portion of the arch, the descending and the sigmoid flexure of the colon.
- The hemorrhoidal plexus is formed by the filaments of the inferior mesenteric, continued around the superior hæmorrhoidal arteries, joined by small branches from the lower lumbar ganglions; it supplies the superior and middle portions of the rectum, and communicates with the hypogastric plexus.
From the sympathetic cords in the thorax a small branch is continued obliquely downwards and forwards on each side, close to the spine, and behind the crus of the diaphragm, to join the first lumbar or abdominal ganglion. This branch is seldom absent; when it is, the inferior splanchnic nerve, after joining the renal plexus, enters this ganglion, so that the continuity is always maintained between the thoracic and abdominal portions of the sympathetic nerves. The lumbar ganglions and their connecting thread are placed on the anterior aspect of the lumbar vertebræ, in a tendinous groove, between the crus of the diaphragm and psoas magnus of either side, nearer the median line above, but diverging below; they are variable in number, usually four, and sometimes only three, and often one is prolongated into another. The external branches of each are two, communicating; they accompany the lumbar arteries, beneath the psoas muscle, close to the grooves on the sides of the vertebræ, and join the anterior lumbar nerves in the intervertebral foramina; they are white and distinct, and may be regarded as the lumbar roots of the sympathetic. These branches frequently have ganglions upon them, and they often unite with filaments from the lumbar plexus.
The anterior and internal branches are aortic and splanchnic. The aortic branches are numerous; they pass forwards in front of the aorta; the nerves of opposite sides unite, and are joined by branches from the solar plexus, and form a plexus, lumbo-aortic. This surrounds the aorta between the superior and inferior mesenteric arteries; small arteries and lymphatic glands and vessels are entangled in it; some of its branches join the inferior mesenteric plexus; inferiorly it divides into three portions; the middle enters the pelvis, and joins the hypogastric plexus; the lateral accompany the common iliac arteries to their division, and several filaments are prolonged around the internal and external iliac vessels. The splanchnic branches pass forwards from each ganglion, and join the several abdominal plexuses already mentioned.
The hypogastric plexus is of considerable extent; it is formed by the continuation of the lumbo-aortic plexus, joined by filaments from the lumbar ganglions; is situated in front of the base of the sacrum, between the common iliac arteries, and divides into a right and left hypogastric plexus; each of these is joined by branches from the sacral ganglions and anterior sacral spinal nerves; each plexus sends off numerous branches, which again form secondary plexuses on the organs to which they are distributed. Thus we have hcemorrhoidal, vesical, prostatic, vesicular, ovarian, and uterine plexuses. All these plexuses contain filaments from the sacral nerves, as well as from the sympathetic, and all are conducted to their terminations by the arteries of each organ.
As the sympathetic cords descend obliquely inwards, over the base of the sacrum, behind the iliac vessels, they are extremely small; in the pelvis, they at first increase in size, descend converging, and each ends in a minute thread; they are placed near the inner margin of the anterior sacral foramina. The sacral ganglions are four or five in number, of an oval or round form; their external branches join the anterior sacral nerves; their internal branches join the hypogastric, or some of their secondary plexuses. From the last ganglion a small branch arches across to meet a similar one from the opposite side: on this a small ganglion (impar) is occasionally to be found; if absent, a connecting plexus occupies its place; the terminal filaments are very minute, and distributed to the fore part of the os coccyx.
Although the sympathetic nerves and their branches appear to differ in structure from the cerebro-spinal nerves, yet they are essentially the same; the fibres seldom appear so white, but have rather a greyish-red color. The general neurilemma of each nerve is more dense, and therefore the internal fibrous or fasciculated texture is not so obvious; but if the former be carefully divided, the latter will be found equally apparent. Tlie great distinction depends on the occurrence of numerous ganglions, both on the principal cords as well as on their branches; each ganglion is invested with a firm capsule, which is continuous with the sheath of the afferent and efferent nerves. This capsule is surrounded by areolar tissue and blood-vessels; the latter ramify on and pierce the capsule; the internal surface of the latter is vascular, and may, on the larger ganglions, be separated as a vascular membrane from the external fibrous layer, and is analogous to the pia mater on the cerebro-spinal axis. The mass of a ganglion is composed of a plexus of nervous filaments, with a variable quantity of vesicular or grey nenrine: the afferent nerves divide into numerous fibrillse, which pass in the most varied directions, and re-unite most probably in different combinations, the interstices being filled with capillary vessels and grey neurine. Whether the efferent nerves consist of those filaments only which composed the afferent, or whether additional fibres are added to these in the ganglion, it is, in the present state of our knowledge, difiicult if not impossible to determine. The only material difference to be observed between the structure of the ganglions of the sympathetic and those of the cerebro-spinal system is, that the latter appear in general to be less red and vascular, and to contain less of the vesicular or grey neurine; the interlacement of white fibres is more obvious in them, and constitutes the greater portion of each, particularly of the spinal ganglions.
Pl. 138, fig. 13, upper part of the great sympathetic nerve: 1, uppermost cervical ganglion; 2, 2, branches from it to the accessory nerve; 3, 3, junctions with the cervical nerves; 4, branch of the vagus; 5, upper branch of the first cervical ganglion; 6, communicating threads to Jacobson’s nerve; 7, threads to the otic ganglion; 8, threads to the oculomotor; 9, threads to the vidian nerve; 10, spheno-palatine ganglion with its branches; 11, pharyngeal and carotid branches of the first cervical ganglion; 12, glosso-pharyngeal nerve; 13, pharyngeal plexus; 17, long or superior cardiac nerve; 18, a cardiac nerve from the vagus; 19, middle cervical ganglion; 20, its upper branches, one of which unites with the first cervical ganglion or with the main trunk, two others with the cervical nerves; 21, middle cardiac nerve; 22, its connecting threads, with the pharyngeal branch of the tenth pair; 23, inferior cervical ganglion; 24, its connexion with the brachial plexus; 25, branches passing into the vertebral canal with the vertebral artery; 26, branches connecting it with the middle cervical ganglion, of which one passes before, the other behind the subclavian artery; 27, lowest cervical ganglion; 28, union of the tenth pair with the cardiac plexus; 29, plexus at the arch of the aorta; 30, plexus between the trachea and the pulmonic artery; 31, tracheal branches penetrating into the lungs; 32, 32, pulmonic plexus (from the tenth pair) and the connexion with the cardiac plexus; 33, anterior, 34, posterior cardiac plexus; 35, 35, two thoracic ganglions; 36, 36, branches to the descending aorta; 37, connexion of a thoracic ganglion with an intercostal nerve; 38, great splanchnic nerve. Fig. 14, lower portion of the sympathetic nerve: 1, 1, 1, three thoracic ganglions, with their roots proceeding from the spinal nerves; 2, 2, branches descending to the aorta; 3, 3, cut branches of the tenth pair to the pulmonic plexus; 4, great splanchnic nerve; 5, lesser splanchnic nerve; 6, 6, solar or cœliac plexus; 7, semilunar ganglion of the right side; 8, vagus of the right side; 9, do. of the left side, with its numerous branches to the stomach; 10, supra-renal plexus; 11, renal plexus; 12, branches to the intestinal canal; 13, aortic plexus; 14, plexus to the seminal organs; 15, 15, two lumbar ganglions, and their connexion with the lumbar nerves and the aortic plexus; 16, 16, two sacral ganglions, connected with each other, and with the sacral nerves, so as to form plexuses about the pelvic vessels; 17, sacral plexus of the spinal nerves.
![]() Organs of Sense
Organs of Sense
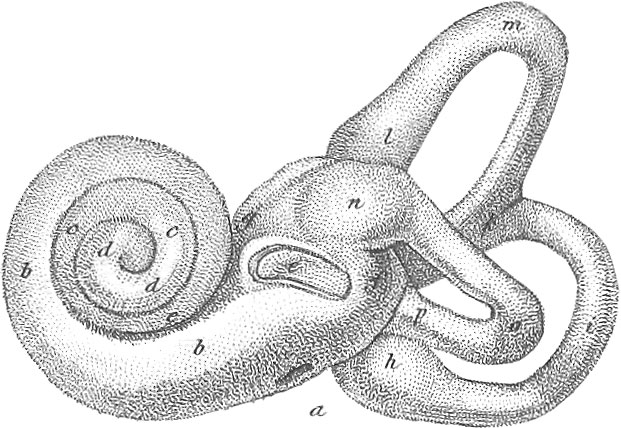 Organs of Sense
Organs of SenseThe organs of the senses establish certain relations between man and the external world, by which he obtains all his knowledge of the physical character and of the general and special properties of all surrounding objects. The organs of sense are all symmetrical, and are usually considered as five in number: the nose, or organ of smell; the tongue, or organ of taste; the ear, or organ of hearing; the eye, or organ of sight; together with the integuments, or the organ of touch. Each organ of sense is placed near the surface of the body, is furnished with an appropriate apparatus suited to its particular functions, and is in direct connexion with the nervous centres. The four first mentioned organs are connected with particular parts of the brain, each by its proper nerve. The sense of touch, however, is distributed over the whole surface of the body, and its apparatus being supplied by the posterior or ganglionic roots of the fifth cerebral and all the spinal nerves, is therefore connected with the cerebro-spinal axis generally.
Anatomy of the Integuments
The seat of the sense of touch, by means of which we become cognisant of such peculiarities of matter as temperature, shape, weight, density. &c., resides essentially in the skin proper, although existing to a considerablo degree in the mucous membranes. Those which are continuous with the skin share with it in the peculiarities of its anatomy, both consisting of two laminæ, one external or superficial, named cuticle, epidermis, or epithelium, the other deeper, and known as the cutis vera or chorion. Beneath the latter is more or less of areolar or cellular and adipose tissue, which serves to support and conduct the numerous vessels and nerves that supply this highly organized structure.
All parts of the skin, and, indeed, most structures in the body, possess a certain degree of sensibility to temperature and to contact, that is, they possess touch generally; but the power of discerning the other qualities of the body is developed only in certain situations where there is a corresponding refinement and development of sentient papillæ, which are enabled to take cognisance of these qualities with a wonderful degree of nicety and perfection. This power of tact, as it has been called, to distinguish it from mere touch, resides especially in the integuments of the fingers and toes.
The office of the skin is not fulfilled merely by serving as an investment to the body, and as the seat of touch. It is the seat of an important secretion which serves to purify the blood in a manner somewhat analogous to respiration. This secretion is discharged in the form of a fine vapor termed the “insensible perspiration;” but when the circulation is increased in. activity, or when the body is exposed to a high degree of temperature, it is given forth in the form of minute drops, which appear like dewdrops upon the surface, and then becomes the “sensible perspiration” or “sweat.” This exhalation carries off from the body a large quantity of water, carbonic acid, saline, and various animal or azotized matters, which are effete or injurious to the system. The importance of a free escape for this cutaneous exhalation is well known. The skin is also the seat of a sebaceous or oily secretion, which preserves it in a soft or pliant state, repels external moisture, and defends it from the drying influence of the air. The skin is also an inhalant and absorbent surface, as shown by its numerous lymphatics arranged in a plexiform manner, and by the fact that immersion in water increases the weight and relieves the thirst. Nutritive substances have even been supplied to the body through the skin, and certain liquids applied to the surface have been subsequently detected in the urine.
To fulfil all these important functions, we find in addition to the three essential elements, namely, the protecting epidermis, the chorion, and the areolar fibrous tissue, that there are superadded numerous glands and follicles, the sources of the perspiration and sebaceous secretion. There is also an extensive and minute capillary net-work of arteries, veins, lymphatics, and nerves. The latter are principally derived from the cerebro-spinal system; and so universally distributed are the vessels and nerves, that the smallest spot on the surface cannot be punctured with the finest instrument without the discharge of blood and the sensation of pain. There are also certain appendages to the skin, as the hair and nails, which will be considered in their proper place.
1. The Cuticle or Epidermis appears to be a thin, semi-transparent, grey lamina, hard, dry, horny, and homogeneous. When minutely examined, however, under water, its deep surface is found to be soft and moist, and numerous fine filaments may be seen to pass between it and the cutis vera. These are probably the elongated and ruptured extremities of the exhalant and sebaceous ducts, together with the sheaths of the fine hairs which invest almost its entire surface. The epidermis is composed of hard, dry laminæ, in each of which may be observed one or two opake spots, the original nuclei and nucleoli of the cells, of a polygonal or irregular form, overlapping each other and adhering to subjacent softer scales. As the scales on the surface become more dry and thin they peel off, and pags away as particles of dust, or bran-like scales, as seen on rubbing the skin with a coarse towel or hair mitten. The deeper structure of the cuticle consists of softer scales or flattened cells, and the portion in immediate contact with the true skin is in an almost semi-fluid state, containing cells and nuclei. This fluid lymph or blastema contains numerous cell germs or cytoblasts, which gradually enlarge into cells which lie close together, and cover every portion of the papillary surface of the cutis. As soon as the first layer is formed, a second is formed immediately beneath it, separating it from the true skin, and causing its drying and desquamation. The superficial scales adhere by their edges; the middle laminæ of cells by their surfaces, the deep-seated are supported immediately by thin blastema.
Granules of coloring matter are found distributed among the deeper cells and in the connecting lymph, and it is upon the amount and tint of these that the complexion of the skin depends. In the Negro and other dark-colored races, this coloring matter appears as a layer of pigment; it is not, however, a distinct or organized membrane, but merely coloring matter deposited in the interstices of the cells; as the latter approach the surface, any coloring matter they carry along with them is lost as they become dry. and hard, partly by evaporation, partly by undergoing some chemical change.
The cuticle being itself insensible and unvascular, forms a most useful investment to the body, defending a highly sensitive surface from pressure and friction, and from the stimulating effects of the atmosphere. It is alsoinvaluable in resisting the evaporation of the fluids of the cutis.
2. Dermis, Chorion, or Cutis Vera. This is composed essentially of areolar tissue condensed into a firm, compact membrane, in which is interwoven more or less of the yellow elastic fibrous tissue, with numerous vessels and nerves. Its inferior surface is loose, open, and cellular, connected and continuous with the areolar tissue of the subjacent parts without any very exact limitation or distinction; the subdermoid cellular tissue contains the cutaneous glands and hair bulbs, and the vascular and nervous ramifications which are to supply the dermis, as also more or less of adipose tissue. This subcutaneous adipose tissue or fat differs in different individuals, according to age, sex, and constitution; it is usually softer and more abundant in the female, and at its maximum in the child.
In the dermis, the upper portion, called the superficial or papillary lamina (although not a separate layer), presents a condensation of the areolar tissue into a smooth membranous surface which is exquisitely vascular and sensible, and presents beneath the epidermis numerous minute elevated lines called papillæ. This lamina is the seat of a vascular capillary plexus, and in the living body appears uniformly red when the cuticle has been detached. The papillæ are studded over this surface, varying in number and size in different parts of the body; the tactual sensibility of different parts of the body is in proportion to the abundance and size of these papillne. Thus on the lower surface of the fingers the skin presents numerous curved or arched grooves and ridges; each ridge consists of a row of conical papillæ, and into the intervening grooves the epidermis sinks, and the small exhalant pores open. The exact structure of the papillæ is difficult to ascertain; each appears to be an eminence or projection of the superficial laminæ of the cutis, with some portion of the fibro-cellular tissue containing blood-vessels, and most probably nerves. The vessels appear as convoluted loops, and constitute the greater portion of the papillæ; nerves also can be traced through the cutis to each papilla. These accordingly may be considered as the true organs of tact.
The excreting apparatus of the skin consists of glands and follicles, some of which supply the perspiration or sweat, others the sebaceous secretion or oily matter.
The sudoriferous or sweat glands exist in all parts of the body, imbedded in the dermis or the subdermoid tissue. Each consists of a convoluted tube closed at its inferior extremity, the other end becoming the fine exhalant duct which passes in an oblique or spiral course through the cutis and cuticle, and opens by a minute pore; it is lined by a fine epithelium continuous with the cuticle.
The sebaceous glands, though not so numerous as the last, are very generally diffused through all parts of the skin except the palms of the hands and soles of the feet. They are very distinct in the auditory meatus (glandes ceruminosæ), on the inner aspect of the eyelids (glandes Meibomianæ), also on the scalp, face, and tip of the nose, around the nipples, and about the anus, scrotum, and corona glandis (glandes odoriferæ). They are small, round bodies, imbedded in the dermis; some are simple, soft, convoluted tubes, others are firm and lobulated. In the scalp and other parts where the hairs exist, one or more of them open into the hair follicles. A minute parasitic animal, the Demodex folliculorum, has been found to inhabit these ducts exclusively. The sebaceous secretion serves to keep the surface moist, soft, and pliant, and in particular situations, as in the ear, eyelids, nipples, &c., it answers special purposes; it also co-operates with the sudoriferous glands in separating hydro-carbonous matters from the blood.
The hair and nails are appendages of the skin, but are rather modifications of the cuticle than allied to the true skin.
3. The Nails cover the dorsal surface of the last phalanges of the fingers and toes, and have a tendency to extend around the extremity of each. They are strong, elastic, insensible plates, curved or concave so as to fit closely the cutis; the root and borders are concealed and fixed in a narrow deep fold in the cutis, termed the nail follicle; the exposed portion or body is convex and ends in the free margin. The surface of the cutis to which the body of the nail adheres is called the matrix, and is so vascular that the red color is seen through the nail; at the root and a short distance beyond it, it is less vascular and more dense, and causes the semi-lunar white spot at the base of the nail, called the lunula. The absence of this lunula is said to characterize the colored races, as distinguished from the white. In the follicle, at the root and borders, are a number of papillæ which form the nail by secreting the blastema in which are formed cell germs; these become flattened and compressed, dry, and harden into nail. As the nail elongates, it thickens by additions to its concave surface from the matrix, and increases in breadth by secretion along its borders. The cuticle is continuous with the nail a little beyond its root and lateral borders, and is also continued from the back of the pulpy end of the finger to its concave surface near the end or free edge; as the nail is thus continuous with the cuticle, so is the matrix with the adjoining cutis. The nails not only protect the sensitive ends of the fingers, but aid them as instruments of prehension, as well as in various manual operations; they also afford a firm point of support behind the tactile papillæ, which is of essential service in the exercise of touch.
4. The Hairs. These cutaneous appendages, like the epidermis and nails, are insensible and non-vascular; they exist in all parts of the body except the palms of the hand and soles of the feet, varying very much in strength, form, color, and extent, in different situations. On the greater portion of the body, they are short, soft, and downy; on the head, in the eyelids, axilla, and on the pubic region, they are much longer and stronger; the extent, however, of their development varies with the age, sex, and temperament of the individual. The loose or projecting portion of a hair is called the shaft; the root is fixed in a follicle composed of an involution of the cuticle and of the superficial lamina of the cutis; this follicle is depressed through the cutis, enlarges into a pyramidal or bulbous form, and is imbedded in the areolar or adipose tissue, from which it receives its vessels, and in which it is so firmly implanted as not to be disturbed by pulling out the hair. The whole follicle is lined by the involuted skin, and at the bottom the cutis presents a highly vascular papilla or pulp, which secretes the matter of the hair. Thus the vessels of the pulp give out the lymph containing cell germs; these become cells with nuclei, and are gradually condensed and elongated into a scaly fibrous substance which is continually pushed forwards by additions from beneath, and escapes through the opening in the epidermis, generally in a slanting manner. The cells forming this outer surface or cortex of the hair are flat and hard, and inclose a more loose fibrous texture named the medulla or pith; these external scales are successively produced, the last formed overlapping the preceding. Owing to the less density of the internal cells, the hair when magnified has a cellulo-tubular appearance. Thus the hair is nothing but cuticle specially modified by the papilla on the cutis vera at the bottom of the follicle. Pigment granules are also intermingled with and adherent to the cells at the root of each hair; on these the color of the hair depends. Into the hair follicle one or more sebaceous ducts open, the secretion of which lubricates the hair and imparts to it its oily character.
5. The Subcutaneous Cellular Tissue is a soft, extensile substratum of the skin, composed of contractile fibres and plates of cellular membrane. It serves to connect the skin with the subjacent fascia, and to conduct vessels and nerves to the true skin; it incloses angular cavities or spaces intercommunicating freely, and filled during life with a watery exhalation.
6. The Adipose Tissue at one time was supposed to be identical with cellular. It is, however, characterized by consisting of numerous short sacs having no opening or communication, each sac being a delicate simple membrane, supplied with blood-vessels and secreting from its cavity the substance called fat. In tLe cellular or areolar tissue, on the other hand, we have numerous bands or threads of white fibrous tissue crossing each other, and leaving interstices which communicate freely. The two tissues are usually associated together, the adipose being inclosed in the meshes of the areolar, but in some situations, as in the medullary canal of the long bones (where it is known as the marrow), in the omenta, along the mesenteric vessels, and upon the heart, the adipose tissue may be abundant, with little or no cellular.
Adipose tissue consists of two distinct elements, the secreting membrane and the secreted product. The former consists of fine transparent membranous cells surrounded by capillaries; each sac is somewhat round, but by aggregation and consequent compression is made to assume various figures. The vessels pass in the interstices between the cells, and surround each by a delicate inosculation. The adeps or fat, which occupies each cell, is a soft, yellowish, oily substance, presenting a great variety with the individual. In youth it is most abundant towards the exterior, the reverse existing in old age. The fat contributes to the covering of the body, and being a bad conductor of heat, assists in retaining its temperature; by filling up numerous interstices, it adds to the compactness and symmetry of the system; it may also serve as a reservoir of nutritive materials from which the system may derive an occasional supply.
Pl. 129, fig. 24, vertical section of the skin showing its microscopical structure: 1, epidermis with its undulating lines; 2, sudoriferous gland and canal; 3, cutis vera; 4, apparatus for secreting pigment substance; 5, sebaceous gland with its duct; 6, 6, papillæ; 7, blood-vessels of the skin. Fig. 25, vertical section of the thumb to exhibit the insertion of the nail: 1, nail; 2, 2, continuation of the cuticle; 3, cutis vera; 3, (left hand side), adipose tissue; 4, fold of skin containing the root of the nail; 6, section of the terminal bone of the thumb. Fig. 26, body of the thumb nail: 1, lateral fold; 2, ridges caused by the linear rows of papillæ on the subjacent cutis vera; 3, lunula or spot at the base of the nail.
Anatomy of the Nose, or Organ of Smell
The nose is situated between the orbits, above the mouth and glottis, and in front of the pharynx and of each tympanum, communicating with all these regions. Though median in position it is really a double organ, being completely divided by a partition or septum into two symmetrical portions, called the nares or nasal fossæ. The nasal passages have a two-fold use: they constitute the organ of smell, the olfactory nerve being distributed to the vascular membrane covering their irregular and convoluted aspect; and secondly, they serve as avenues to the respiratory organs. We may conveniently examine the nose as composed of two portions: the one, anterior or external (the nose proper), consisting of cartilages and soft parts; the other, posterior or internal, the nares or nasal fossæ, composed of bones covered by highly vascular mucous membrane.
The Nose is essentially formed of cartilages; one occupies the median line or septum, the others are placed on each side and form the alas. They are continuous laterally with the superior maxillary, and superiorly with the margin of the nasal bones; inferiorly they bound two oval openings, the nostrils. Each nostril has its long axis, antero-posterior, and is partly surrounded by stiff hairs (vibrillæ) which bend across it and instantaneously give notice of the entrance of foreign particles. The skin covering the tip of the nose is thickened, and furnished with numerous sebaceous follicles, the mouths of which frequently appear like black dots, owing to the adhesion of extraneous particles. The secretion of these follicles may often be forced out in fine long threads like small worms.
The cartilages of the nose or fibro-cartilages are five in number, one in the centre, one at each side, and one inferiorly in each ala. The septal or median cartilage is a true cartilage of considerable strength; it not only separates the nostrils, but also the anterior portions of the nasal fossæ. It is inclosed in thick mucous membrane, and is not always vertical, but may project to one side.
The lateral nasal cartilages are two on each side, superior and inferior. The superior lateral is attached externally and posteriorly to the nasal process of the superior maxillary bone and to the inferior margin of the nasal; anteriorly and internally to the opposite one and to the septal cartilage, and inferiorly by fibrous tissue to the inferior cartilages. The inferior lateral or alar cartilages form the upper part of each ala, the tip or lobe and the boundary of the nasal openings. All the lateral cartilages are readily acted on by the superimposed muscles, which can move the whole organ, or alter the shape of the openings, but cannot perfectly close them.
Pl. 132, fig. 29, left side of the nose of an adult, the cuticle supposed to be removed for the purpose of more clearly exhibiting the openings of the sebaceous follicles. Fig. 30, lateral view of the bones and cartilages of the nose: a, a, skin of the nose; b, left nasal bone; c, left superior lateral cartilage; d, left alar cartilage with its three appendages, e, f, g, which are attached to each other by the ligaments h, i, k. Fig. 31, anterior view of the nasal cartilages: a, b, nasal bones; c, d, superior lateral cartilages; e, septum; f, f, small cartilages proceeding from it; g–o, alar cartilages with their three appendages. Fig. 32, outline view of the preceding figure. Fig. 33, inferior view of the nasal cartilages: a, b, c, d, outline of the nose: e, septal or median cartilage; f, extremity of the upper jaw to which it is attached; g–k, alar cartilage of the left side with its three appendages; l–o. do. of the right side. Fig. 34, superior lateral cartilage of the nose. Fig. 35, septal cartilage of the nose. Fig. 36, left alar cartilage. Fig. 37, do. with its three appendages (from without). Fig. 38, do. from within. Figs. 39 and 40, the three small cartilaginous appendages, without and within.
The Nasal Fossæ are bounded by several bones which are covered by a very delicate periosteum; to the anterior part of the bones of the nose are attached the cartilages already described. These several bones are the nasal, frontal, ethmoid, sphenoid, superior maxillary, palatine, unguis, spongy, pterygoid, and vomerine bones. The external wall of each naris is deeply grooved by three fossæ, the superior, middle, and inferior meatus; these are situated between the spongy bones, the middle being the widest. The nasal or lachrymal duct opens into the anterior third of the inferior meatus, the Eustachian tube behind. Into the middle meatus the antrum maxillare opens by a small oblique slit, in front of which is a groove named the infundibulum, leading from the frontal sinus; into this groove the anterior ethmoidal cells open. The posterior ethmoidal cells and the sphenoid sinuses open into the upper meatus. Each naris opens posteriorly into the pharynx above the velum, by an oblong oval opening, separated from each other by the vomer.
All the internal surface of the nose and of the communicating sinuses is lined by a soft, vascular, and highly sensitive mucous membrane; this is the pituitary or Schneiderian membrane. The olfactory nerves are distributed to it on the septum and ethmoidal region in the form of numerous plexuses; it is also supplied on each side and on the septum with branches from the ophthalmic and superior maxillary divisions of the fifth pair. The olfactory or first pair of nerves endow the superior portion of this membrane with its peculiar sense or power of smelling; while its general acute sensibility depends on the fifth pair, the general nerve of feeling of the head.
Such bodies can alone be considered as capable of imparting the sensation of smell as are capable of being vaporized or dissolved in the atmosphere. The essential conditions of smell, however, are not yet satisfactorily ascertained; so much is certain, that the odorous particles must come in contact with the nerves, and especially by being inhaled in ordinary nasal respiration. If the breath be held, no perception of odor takes place, and if a piece of camphor be held in the closed mouth during nasal exhalation, comparatively little odor will be perceived. The particles of matter, nevertheless, do not come into immediate contact with the nerves, since the mucus of the nose is interposed, together with the basement membrane of the Schneiderian. It may be that solution in the mucus is necessary to this sense, as when the nasal passages are dry it is much enfeebled.
Pl. 132, fig. 27 a, a portion of the Schneiderian membrane with its nerves of natural size; fig. 27, b, the same magnified three diameters: a, b, dura mater; c–f, section of the Schneiderian membrane; g, g, section of the cribriform plate of the ethmoid bone; h, h, foramina in it for the transmission of nervous filaments; i, branch of the olfactory nerve, cut off to show the following branch k, with the manner of its escape from the dura mater l, and the passage of the nerve through the bone m; n, o, p, arteries of the Schneiderian membrane. Fig. 26, distribution of the olfactory nerve on the septum of the nose: a, b, c, d, nerves of the olfactory; e, nervous branch from the fifth pair; f, g, superior posterior nasal nerves from the second branch of the fifth pair; h, superior cutaneous nasal nerve, from the infraorbital nerve; i, k, apparent boundary of the branches of the olfactory nerve. Fig. 28, nervous plexus of the lining membrane of the nose: 1–8, basal extremities of the first eight cerebral nerves; a–d, olfactory bulbs with their threads, 12, 13, passing through the cribriform plate; 9 to 12, larger portion of the fifth pair of nerves; e, f, g, first branch of the fifth pair. h–k, second branch. Figs. 41 and 42, two sections of the nasal cavities: fig. 41, the lower, fig. 42, the upper: a, outline of the nose; b, c, nasal bones; d, e, frontal bone; f, g, h, i, ethmoid bones; g, i, k, l, alar process and sphenoid bone (cut edge); r, r, middle lamina of the ethmoid bone (cut edge); s, s, and t, t, thickness of the mucous membrane of the nose; u, u, length and breadth of the left, v, v, of the right nasal cavity; w, w, x, x, cells of the ethmoid bone; y, z, membrane reflexed. Fig. 43, posterior surface of a vertical section of the nose; a, b, nasal cartilages; c, c, septal cartilage; d, d, Schneiderian membrane; e, e, hairs and mucous glands; f, g, nostrils. Fig. 44, posterior sectional surface of the nasal cavities: a–f, cut edge of various bones; g, h, lachrymal sac and lachrymal duct opening into the inferior meatus; i, k, l, m, section of the Schneiderian membrane; n, n, the surface of the membrane turned towards the nasal cavity; p, q, lachrymal sac and lachrymal duct of the left side; r, r, inner bony wall of the maxillary sinus. Fig. 45, posterior sectional surface of the nasal cavities and the communicating sinuses: a, b, frontal bone; c–l, ethmoidal; m, n, left and right superior turbinated bones; p, p, vomer; q–y, upper jaw; a, f, Schneiderian membrane; g, g, opening of the left lachrymal canal; h, opening of the right; k, l, m, opening of the maxillary sinus on the right side, m is a probe introduced; n, o, p, section of the periosteum of the orbit; s, section of the soft palate; 1–6, teeth.
Anatomy of the Ear, or Organ of Hearing

By means of the sense of hearing an animal is enabled to take cognisance of sounds and of all their variations. Sound is the result of any impulse conveyed to the organs of hearing, by undulations of air, these organs being so constructed as to receive these undulations, and so organized as to become sensible to them and to convey the impressions to the sensorium. This sense, next to vision, is most valuable to man, as forming the bond of social union and the great inlet for all knowledge conveyed by voice and language. Each organ consists of a special nerve expanded on membranes, and endowed with the properties of sensibility to the varying impressions of sound and of conveying these impressions to the sensorium; and secondly, of a physical apparatus fitted for receiving, conducting, and in some measure regulating these impulses in their course to the sentient nerve.
We may divide the ear into an external, middle, and internal portion. The external comprises the auricle, commonly called ear, and the external meatus or tube; the middle consists of the tympanum or drum with its chain of small bones; and the internal or true ear is called the labyrinth, and comprises the vestibule, cochlea, semicircidar canals, meatus auditorius internus, and auditory nerve. This portion is lodged in the petrous division of the temporal bone, and is thereby protected from external pressure or injury.
External Ear
The external ear, or auricle, is situated at the side of the head: it consists of the auricle or pinna and the external meatus, which terminates at and is closed by the tympaum.
The Pinna, or Auricle, commonly termed the ear, is the external portion, composed of cartilage, ligament, and a few muscular fibres, the whole inclosed in a duplicature of the skin. It is convex towards the head, and concave externally, in which aspect it presents various irregularities, all tending towards the meatus. The convex border which forms the outline of the ear is called the helix; superiorly this edge is thin, and curled outwards so as to bound a depression named the fossa innominata; anteriorly it bends downwards and backwards into the concha and above the meatus. Anterior and inferior to the helix is the semicircular prominence called the antihelix. This is narrow and prominent behind; as it ascends it becomes broader, retires from the surface, and divides into two crura, which run in beneath the edge of the helix; this depression between its crura is named the scaphoid or navicular fossa. Anterior to and overhanging the meatus auditorius, somewhat like a valve, is the eminence called tragus, of a triangular form. The free apex of this is directed towards the concha, and the inner surface is beset with strong coarse hairs or vibrillse, which extend across the orifice of the meatus. When pressed backwards or inwards, the tragus can cover the meatus. Opposite to the tragus and separated from it by a deep round notch is the antitragus, a small tubercle connected with the lower extremity of the antihelix. Within the antihelix, tragus, and antitragus, and traversed above by the helix, is the large and deep depression called the concha, into which all the other grooves converge; it leads directly downwards into the meatus. The lower pendulous part of the auricle is called the lobe, and contains none of the cartilage which constitutes the skeleton of the rest of the ear.
The ligaments of the auricle are the anterior, from the root of the zygoma to the anterior part of the helix, and to the tragus; and the posterior, from the mastoid process of the concha.
Of the muscles of the external ear we have already considered those which move it on the head (anterior or attrahens, superior or attollens, and the posterior or retrahens). The intrinsic muscles, or those which only pass from one part of the cartilage to the other, are named from the eminences to which they are attached. They are the major and minor helices, the tragicus, anti-tragicus, and transversus auricularis. These muscles, though only rudimentary in man, are highly developed in some of the inferior animals.
Meatus auditorius extermus is a tube leading from the concha to the membrana tympani; it is about an inch and a quarter long, with the external half of cartilage, the remainder of bone. By drawing the auricle upwards and backwards we can partly straighten the canal, and, with a strong light directed in it, we can see down to the membrana tympani. The bony portion of the meatus is wanting in the child, its place being supplied by a mere ring. The auditory canal is lined by the integument, continued from the auricle; the cutis ceases at the margin of the lower extremity, but the cuticle is continued over the membrana tympani. The skin, from a little distance within the external orifice to within a quarter of an inch of the tympanum, is perforated by numerous small openings, the openings of the sebaceous follicles and of the ceruminous glands. These glands secrete the. cerumen, or ear wax.
Middle Ear
The middle ear or tympanum is the space within the membrana tympani, external to the osseous walls of the vestibule and labyrinth, in front of the mastoid cells, and communicates anteriorly with the Eustachian tube. It contains air and a little fluid, and is traversed by the chain of small bones, and by fine nerves and vessels. Its walls are lined by a fine mucous membrane, continuous through the Eustachian tube with that of the nose.
1. Membrana Tympani. This is situated at the inner and lower extremity of the meatus, separating it from the cavity of the tympanum or drum, the outer wall of which it forms. It is a thin, dry, semi-transparent membrane, nearly circular, with the vertical diameter a little longer than the transverse or antero-posterior. The inner surface of the membrana is directed upwards and inwards, and adheres intimately to the handle of the malleus bone. Although thin and semi-transparent, the membrana tympani consists of three distinct layers, an external or epidermis, an internal or mucous, and a middle or fibrous. We have already referred to the two former; the latter presents the appearance of fibres radiating from the exterior to the malleus, into which they are inserted.
The internal or vestibular side of the tympanum presents several points of observation. At its upper part is situated the kidney-shaped foramen, fenestra ovalis or vestibuli. This is directly opposite the membrana tympani, and in the dry bone leads to the vestibule; in the recent state it is closed by a membrane. The base of the stapes also closes this opening. Below the foramen ovale is the bony projection of the promontory, which corresponds to the first turn of the cochlea, and on the surface of which there are delicate grooves converging below to a common canal, which transmits the nerve of Jacobson from the glosso-pharyngeal nerve. Behind the fenestra ovalis is the bony pyramid, the apex of which is perforated by a small canal. Below and behind the promontory is the foramen rotundum or fenestra cochleæ, which in the recent state is closed by membrane.
The posterior wall of the tympanum presents a large irregular opening at its upper part, leading into the mastoid cells. The anterior wall tapers off into the Eustachian tube, above which are the cochlear! form osseous plate and the canal for the tensor tympani muscle.
2. The Eustachian Tube is a narrow canal, about an inch and a half long, leading from the tympanum obliquely towards the back of the nose, where it opens on the side of the pharynx and on a level with the inferior spongy bone. The tympanic portion is chiefly osseous; the remainder is composed of cartilaginous, fibrous, and mucous tissues. The use of this tube is to admit external air into the tympanum, by means of which the membrane is enabled to resist the pressure of the atmosphere; it also serves to conduct the secretions of the tympanic cavities into the fauces.
The tympanum also presents another small opening or canal, anteriorly and inferiorly, which leads to the inner side of the fissure of Glasser, and transmits the chorda tympani nerve. The cavity of the tympanum is traversed by a chain of small bones, one attached externally to the membrana tympani, and another to the membrane in the fenestra ovalis.
3. Ossiculi of the Ear. The small bones of the ear are three, or according to some, four in number, and are named from a fancied resemblance, malleus or hammer, incus or anvil, and stapes or stirrup. The fourth, or orbicular, is by many considered a mere epiphysis to the long leg of the incus.
Malleus is immediately within the membrana tympani, and connected to, it; it presents a head, neck, manubrium or handle, and long and short processes. The head presents an articulation for the incus.
Incus is placed internal and posterior to the malleus, and bears some resemblance to a bicuspid tooth; it presents a body or head, and a short and long crus. The body is lodged in the recess of the tympanum, and receives the head of the malleus in its deep concave surface. The short crus occupies the opening into the mastoid cells. The long crus descends vertically in the tympanum, parallel to the handle of the malleus. At its extremity is the round tubercle, which is sometimes united to it like an epiphysis, and at others separable from it, when it is called os orbiculare or lenticulare.
The stapes, or stirrup, is placed horizontally between the crus of the incus or orbicular bone, and the fenestra ovalis, to the membrane of which its base is attached. Its head presents a small cavity for articulation with the orbicular bone, or with the crus of the incus; its base is a thin plate, closing the fenestra ovahs.
The articulations between these three bones are furnished with synovial membranes and capsular ligaments, and are further secured in their places by three ligaments. One extends from the head of the malleus to the upper wall of the tympanum; another connects the short process of the incus with the opening of the mastoid cells; and a third extends from the margin of the fenestra ovalis to the margin of the base of the stapes.
4. Muscles of the Tympanum are only two in number, the stapedius and the tensor tympani. The stapedius arises within the pyramid, and is inserted into the back part of the neck of the stapes. The tensor tympani is a very distinct and long fibro-muscular cord, chiefly lodged in the bony canal above the cochleariform process and Eustachian tube. It arises from the cartilage of that tube, and from the adjacent portion of the sphenoid bone. It is inserted into the inner, anterior, and superior portion of the handle of the malleus. The use of the stapedius muscle is not well ascertained; that of the tensor tympani is to draw the handle of the malleus inwards and forwards, by which the membrane is rendered more tense. Two other muscles, laxator major and minor as described by some authors, appear to be only ligamentous fibres.
Pl. 132, fig. 1, left ear: a–e, helix; f–k, antihclix; l, tragus; m, anlitragus; n, lobe of the ear; o, p, depressions between these elevations; q, concha. Fig. 2, muscles of the ear: a–e, cartilages of the ear; f–p, elevator or attollens; q–t, attrahens; u–z, two retrahens. Fig. 3, small muscles on the outside of the ear: a b c, greater; d e f, smaller muscles of the helix; g, h, muscle of the tragus; i, k, muscle of the anti-tragus. Fig. 4, muscle of the inside of the external ear: a–f, transverse muscles of the ear. Fig. 5, section of the tympanic cavity: a, meatus opened; b, fossa on the inferior wall of the meatus; c, fold for the membrana tympani; d, d, tympanic cavity proper; e, entrance into the mastoid process; f, cells of do.; g, promontory; h, fenestra ovalis; i, Fallopian canal; k, superior semicircular canal; l, mastoid process. Fig. 7, membrana tympani from the inside: a, annular fold into which it is fastened; b, malleus; c, elevation; d, d, fibres of which it consists. Fig. 8, ossicles of the ear in their proper positions: a–d, temporal bone; e, tympanic ring; f, malleus; g, incus; h, stapes. Figs. 9 and 10, malleus from two directions magnified: a, long process or gracilis: b, short process; c, manubrium; d, neck; e, head; g, articulating face for the incus. Figs. 11 and 12, incus: f, body; g, short process or crus; h, long or inferior crus; i, os lenticulare; k, articulating face for the malleus. Figs. 13 and 14, stapes: a, b, head; c, neck; d e g, crura; f, base. Fig. 15, temporal bone: a, b, Eustachian tube; e, f, tensor tympani; g, h, i, stapedius muscle.
Internal Ear
This is the essential part of the organ of hearing. It lies deeply buried in the petrous bone, and consists of a number of curiously formed channels and spaces wrought out of the osseous structure, and containing delicate membranous tubes filled with fluid. On these the terminal branches of the sentient nerve are expanded. The internal ear or labyrinth consists of two portions, an osseous and a membranous. The osseous labyrinth consists of three distinct compartments: one in the centre, termed the vestibule; one behind this, composed of three semicircular canals; and one in front of it, the cochlea. Both the anterior and posterior compartments communicate with the vestibule; and the meatus auditorius internus communicates with each of these by minute foramina for the transmission of the auditory nerve.
1. Meatus Auditobius Internus is shorter and smaller than the external. It is scarcely a quarter of an inch in length, and, lined by the dura mater, it leads from the cranium directly outwards, ending in a cul de sac, subdivided into two by a horizontal bony crest. In this depression are seen various minute foramina for the transmission of the nerves.
2. The Vestibule, or central cavity of the labyrinth, is a very small space placed between the fenestra ovalis and the meatus auditorius internus. Its form is very irregular, owing to dilatations in three directions, these bearing the names respectively of superior ventricle or cornu, inferior and posterior, and inferior and interior. In each cornu there are certain openings. On the tympanic side of the vestibule is seen the fenestra ovalis, closed by membrane and the base of the stapes. The inner or cerebral wall of the vestibule corresponds with the base of the meatus internus. It is cribriform, and transmits some fibrillæ of the auditory nerve, and some fine capillary vessels. In the posterior and lower horn are seen three distinct foramina, the orifices of the semicircular canals. In the superior cornu are the two other openings of these tubes. In the inferior and anterior cornu is a distinct oval opening, which leads downwards and forwards into the vestibular scala of the cochlea. Thus there are seven large foramina in the vestibule. The smaller foramina are: 1, those in the cribriform lamina for the auditory nerves; 2, the aqueductus vestibuli, which opens in a suture on the posterior wall internal to the common opening of the semicircular canal, and transmits a small vein. In the anterior horn there is a depression (fossa hemispherica), cribriform, for the passage of nerves. It is separated from another cribriform depression (fossa elliptica) by a prominent bony ridge (eminentia pyramidalis).
3. Semicircular Canals are three long tubes imbedded in the petrous bone, behind the vestibule, and communicating with it. They are curved so as to form nearly three fourths of a circle. They open by each extremity into the vestibule; two, however, unite by their adjoining extremities, so that but five openings are presented. Two of these canals have a perpendicular, and one a horizontal direction.
4. The Cochlea is the most anterior part of the labyrinth, and is a very complicated apparatus. It derives its name from a strong resemblance to the shell of a snail. It may be considered as a tapering tube, closed at its smaller extremity, coiled round a central pillar, the tube itself being subdivided by a partition into two semi-cylindrical tubes. It presents for notice, the tube, the lamina spiralis, the axis or modiolus, and the scalse.
The tube is about an inch and a half long, and descends two turns and a half The second turn lies, at its beginning, within the first, but near its end rises above it. The axis or modiolus is a conical tube, whose summit is expanded like a funnel. It arises from the base of the cochlea, and is directed almost horizontally outwards: the coils of the cochlea and of the lamina spinalis twine round it. The whole of this axis is concealed by the tube of the cochlea; its base or origin is pierced with foramina for the auditory nerves. The apex is expanded into the infundibulum. The centre of the modiolus is traversed by canals for branches of the auditory nerves and blood-vessels.
The lamina spiralis is a very thin plate of bone wound spirally, like the turns of a screw, round the modiolus, into which its inner margin is inserted. In the dry bone, the outer margin is free, but in the recent state it is continued by membrane to the opposite and outer walls of the tube. If unwound and separated from the modiolus, it would present the appearance of an elongated isosceles triangle. The apex of this stands out from the modiolus in the form of a hook (the hamulus of the lamina spiralis). The lamina is composed of two thin plates, between which the cochlear vessels and nerves are distributed.
The two secondary cavities into which the cochlear tube is divided by the lamina spiralis are called scalæ. The superior is called vestibular scala, from communicating directly with the vestibule; the other is the scala tympani, and communicates with the tympanum through the fenestra rotunda. Although elsewhere separated, the two scalæ communicate near the summit of the cochlea by a common opening called helicotrema. Near the termination of the scala tympani at the fenestra, is the opening of the aqueduct of the cochlea, a canal for a small vein.
Membrane lining the labyrinthic cavity. This is an extremely delicate membrane, of a fibro-serous character. One surface is closely adherent to the bone, like a periosteum; the other is smooth, and secretes the perilymph or aqua Cotunnii, a semi-fluid substance.
5. The Membranous Labyrinth. This is not so extensive as the osseous labyrinth, as it does not enter the cochlea. It is separated from the walls of the osseous portion in which it occurs by the perilymph. The membranous labyrinth is itself filled by a liquid called endolymph or liquor of Scarpa. The labyrinth consists of the common sinus, the sacculus, and the membranous semicircular canals.
The common sinus or vestibular ventricle is an elongated, laterally compressed pouch, which occupies the posterior part of the vestibule; the semicircular canals are continuous with it, and open into it by fine orifices; it floats in the perilymph, and is distended by the endolymph.
The sacculus vestibuli is much smaller than the sinus; it is round and situated inferior and anterior to the sinus, to which it adheres; anatomists are not agreed as to whether the two communicate or not.
The membranous semicircular canals have precisely the same form as the osseous canals, presenting the same number of ampullæ or ovoid vesicles. They are surrounded by perilymph and distended by endolymph. The otolithes of certain fishes are represented in man by a powder composed of carbonate and phosphate of lime, and known as otoconia. The grains composing this powder are supposed to play an important part in the physiology of hearing, by communicating to the nervous expansion a more vivid and energetic impression than a single liquid could effect.
6. Nerves of the Ear. The essential nerve of sense is the portio mollis of the seventh pair, or the auditory nerve proper. This enters the meatus internus, and at the bony crest at the bottom of this canal divides into two branches, an anterior, larger, for the cochlea, and a posterior for the vestibule and semicircular canal. The vestibular nerve immediately separates into three sets of fasciculi, superior, middle, and inferior. The superior pass into the superior ventricle of the vestibule, and are expanded on the sacculus communis and on the ampullæ of the semicircular canals. The middle set pass through the macula cribrosa into the anterior ventricle, and expand on the sacculus proprius; while the posterior set pass through the posterior wall of the vestibule, and are lost on the ampullary dilatation of the oblique semicircular membranous canal.
The cochlear nerve resembles a flat tape rolled on itself lengthwise. It passes downwards to the depression at the bottom of the internal meatus, where it divides into a number of fine filaments, which enter the small bony canals leading into the substance of the axis, and pass out between the osseous plates forming the lamina spiralis. The nerve divides into numerous branches which anastomose with each other, and spread out into a delicate nervous membrane, or according to some, terminate in the form of papillæ.
The facial or portio-dura nerve enters the meatus along with the auditory, and entering the aqueduct of Fallopius passes to the hiatus Fallopil, where it is joined by the superior petrosal branch of the vidian and presents a ganglion enlargement. The corda tympani may be regarded either as the continued petrosal branch of the vidian, or as proceeding from the last-mentioned ganglion. It passes into the ear, winds among the tympanic bones, and escapes by a bony canal in the glenoid fossa. The tympanic plexus is a delicate network, chiefly formed by the tympanic branch of the glosso-pharyngeal nerve, or the nerve of Jacobson.
Having thus considered the general features of the ear, we may proceed to a brief reference to the probable functions of its different parts. The auricle or external ear collects and concentrates the sounds which fall upon it; and by the motion of the head and spine it can be turned in every direction to receive them. The meatus auditorius conducts and reflects from its sides the sonorous undulations to the membrana tympani, which is thereby thrown into vibrations, and these are transmitted by the chain of bones to the membrana vestibuli, and partly to that of the foramen rotundum, through the air and fluid which the tympanum contains. The Eustachian tube, by admitting air into this chamber, favors these vibrations as well as the motions of the ossicula; it may also allow the escape of such sonorous impulses as strike on the walls of the labyrinth, and which might produce an echo or confusion of sound. The mastoid cells may also contribute to this effect as well as lighten the bone. Finally, the impressions impinge on the membranous labyrinth on which the sentient nerves are expanded, and then convey the impressions to the sensorium. Sonorous undulations, which strike the bones of the head and face, and the teeth, are transmitted through these solid structures to the temporal bone, and especially to the cochlea, on which numerous auditory nerves are expanded.
Pl. 132, fig. 16, relation of the ossicles of the ear to the nerves which lie between them: 4, membrana tympani; 6, handle of the malleus; 11, process of the incus: 14, tensor tympani; 5, corda tympani. Fig. 17, Jacobson’s plexus; a, promontory; b, portion of the mastoid process; c, malleus; d, incus; e, stapes; f, fenestra cochleae; g, internal carotid artery; h, Eustachian tube; i, tensor tympani; k, laxator tympani; l, Jacobson’s nerve; m, a recurrent branch of do.; n, branch to the fenestra cochleæ; o, continuation of the main trunk; p, inferior branch for the carotid artery; q, superior branch of Jacobson’s nerve from which passes a thread, r, to unite with the branch, s, to supply the Eustachian tube at t; u, first thread to the fenestra vestibuli; v, second thread; w, branch to the promontory and the Eustachian tube; x, end of Jacobson’s nerve, as the superficial petrosal which finally joins the otic ganglion. Fig. 18, bony labyrinth from above, magnified four diameters: a, b, c, d, cochlea; e–g, vestibule; h, i, k, posterior semicircular canal; l, m, k, superior do.; n, o, p, horizontal do. Fig. 19, bony labyrinth from below, or from the side of the meatus auditorius internus: a–c, base of the cochlea with the small foramina for the passage of vessels and nerves; d, foramina for the nerves of the membranous labyrinth; e, cribriform lamina for the ampullæ; f, foramen for the aqueduct of the vestibule; g, h, i, posterior semicircular canal; i, k, l, superior do.; m, n, o, horizontal do.; p, opening for the nerve of the posterior semicircular canal; q, aqueduct of the cochlea. Fig. 20, labyrinth magnified four diameters to show the distribution of arteries in its interior: a, first coil of the cochlea broken open; b, inner surface covered by the periosteum; c, bony portion of the lamina spiralis in the first coil; d, vestibule; e, canal for the malleus muscle; f, g, h, artery for the labyrinth; k, posterior semicircular canal with its arteries; l, superior do.; m, horizontal do.; n, common opening of the superior and posterior semicircular canal. Fig. 21, general relations of the membranous labyrinth: a, cochlea; b, vestibule; c–f, semicircular canals; g, lamina spiralis; h, edge of the lamina; i, sinus and sacculus of the vestibule; k, l, l*, ampullæ of the three semicircular canals; m, horizontal canal; n, auditory nerve; o, cochlear nerve; p, q, branches to the ampullæ; r, middle branch to the sinus of the vestibule. Fig. 22, labyrinth opened: a–e, lamina spiralis; f, bony, g, cartilaginous portion; h, i, membranous portion; l, space between the sinus and sacculus; m, sinus with which the fine openings of the semicircular canals communicate; n, posterior semicircular canal; o, superior do.; p, horizontal do., all with their ampullæ. Fig. 23, labyrinth from beneath to show the common opening of the superior and inferior semicircular canals, and the course of the auditory nerve: a, cochlea; b, vestibule; c, d, e, posterior semicircular canal; f, common opening; g, horizontal canal; e, h, superior canal; i, facial nerve; k, auditory nerve; l, cochlear nerve; m, nerve for the superior and horizontal semicircular canal; n, nerve to the sinus; o, small nerve for the ampullæ of the posterior canal. Fig. 24, magnified representation of the nerves of the labyrinth in the vestibule and on the ampullæ. Fig. 25, distribution of the cochlear nerve on the lamina spiralis of the cochlea. Fig. 6, connected view of the different portions of the ear; a, external ear; b, c, meatus auditorius; d, attachment of the membrana tympani; e, membrana tympani in its ring; f, g, h, malleus; i, k, incus; m, stapes; n, vestibule; p, superior; q, posterior; r, horizontal semicircular canals.
Anatomy of the Eye, or Organ of Vision

Appendages of the Eye not directly concerned in Vision
In addition to the eyeball proper, with its apparatus of lenses, fluids, and membranes, in which the formation of images occurs, there are various appendages all more or less concerned in protecting the eye, and in enabling it to perform its functions properly and conveniently. These consist of the orbits, eyebrows, eyelids, conjunctiva, lachrymal apparatus, muscles of the eye, and ocular fascia, with their several blood-vessels and nerves.
The Orbits. These are conical bony recesses, the sides of unequal length, and joined to each other at angles so as to form quadrangular pyramids; seven bones enter into their formation, the frontal, sphenoid, ethmoid, malar, maxillary, unguis, and palate. The axis or central line of the orbits leads obliquely from the apex forwards and upwards and a little downwards. If, therefore, the axes of both orbits be produced, they will diverge considerably in front, but meet rapidly behind, intersecting at the back of the body of the sphenoid bone. These lines are not parallel to the axes of the eyeballs, which lead more directly forwards and are nearly horizontal. The foramina in the orbit are: 1. The optic, which transmits the optic nerve, and beneath this the ophthalmic artery. 2. The foramen lacerum superius or sphenoidal fissure, the larger inner end of which corresponds to the axis of the orbit, and transmits the third, fourth, ophthalmic division of the fifth, and the sixth cerebral, and filaments of the sympathetic nerves. Beneath these the ophthalmic vein escapes from the orbit to join the cavernous sinus. The external part of this foramen is closed by membrane, through which a small artery from the middle meningeal sometimes passes and assists in supplying the lachrymal gland. 3. The lacerum inferius or spheno-maxillary fissure is in the inferior external angle of the orbit, and transmits small nerves and vessels from the orbit to the zygomatic fossa. 4. Internal orbital foramina, generally two, but sometimes more, are in the superior internal angle; the anterior transmits the nasal twig of the ophthalmic nerve; the posterior, the ethmoidal branch of the ophthalmic artery.
1. The Supercilia, or eyebrows, bound the superior eyelids; they correspond to the superciliary ridge of the frontal bone, which partly causes their prominence. The hairs of the eyebrows are mostly directed in a slanting manner outwards, and are placed in two rows, the superior directed downwards and outwards, the inferior upwards and outwards; both rows converge in a median ridge, which causes a greater fulness and an even, regular appearance. The eyebrows are of use in shading the eye from very strong light, and protecting it from particles of dust and from perspiration and other fluids. They can be moved in three directions: upwards, by the occipito-frontalis muscle; downwards, by the orbicularis; downwards and inwards, by the corrugators.
2. Palpebræ, or Eyelids. These are the two movable semilunar curtains, or folds of skin, placed in front of each orbit, convex and rounded, with horizontal wrinkles, and exactly moulded to the eye. The opening between them is called the palpebral fissure or rima. When the lids are open, they circumscribe an aperture more or less elliptical, on the size of which the apparent magnitude of the eye greatly depends. Its extremities are called canthi. The outer canthus is an acute angular commissure a little rounded, about a quarter of an inch distant from the edge of the orbit, to which it is attached by a dense fibrous membrane. The inner canthus extends for a short distance inwards towards the side of the nose, the edges being a little rounded; externally it presents a small tubercle on each edge called the lachrymal papilla, the point of which exhibits a minute but distinct foramen, the punctum lachrymale, which is the commencement of a small canal, the lachrymal duct, by which the tears are conveyed into the lachrymal sac and thence into the nose. From between the puncta the palpebral fissure leads inwards and enlarges into a small triangular space, the lacus lachrymalis, in the centre of which there is a red papilla, the lachrymal caruncle, between the upper and lower lachrymal duct. The upper eyelid is much deeper and more movable than the lower. The free or ciliary margins of the palpebræ are thick, firm, and abrupt, cut off horizontally so as to meet closely by flat surfaces.
The palpebræ are composed of skin, areolar tissue, an orbicular muscle, cartilage or fibro-cartilage, with connecting fibrous membrane, glands, and mucous membrane. The upper lid also has a special levator muscle, and the free border of each is fringed with rows of hairs or cilia.
The skin is continuous with that of the forehead and cheek, and is of exceedingly delicate texture. The semilunar concentric folds, seen when the eye is open, are effaced when the lids are closed. The areolar tissue is very fine and loose, perfectly free from adipose structure.
The cilia or eyelashes are stiff and strong, and have curved hairs placed in three or four rows in the cutaneous edge of the free margin; all are curved or bent, the superior upwards, the inferior downwards, so that when the lids are closed the convexities only touch, without the hairs becoming entangled with each other. The cilia defend the eye from the admission of particles of dust, minute insects, &c., and can also shade it in too strong a light. Along the posterior or ocular edge of each free border is a row of minute foramina, the openings of the ducts of the Meibomian glands.
The orbicular or sphincter muscle is the next tissue in the palpebræ; it also extends over the circumference of the orbit, superiorly into the super-cilia, and inferiorly into the cheeks. All the fibres are attached into the internal tendon, the tendo oculi or palpebrarum; this is inserted into the nasal process of the maxillary bone, thence it is directed outwards in front of the lachrymal sac, above its centre, and bifurcates. Each band incloses a lachrymal duct, and is inserted into the inner extremity of each tarsal cartilage beneath the punctum. This muscle closes the lids as a sphincter, by depressing the upper one considerably and raising the lower one very slightly, at the same time drawing it horizontally inwards. It supports the globe of the eye, directs the lachrymal secretion into the puncta, cleans and polishes the surface of the cornea; it also serves to protect the eye from too much light.
The palpebral or tarsal cartilages are thin elastic plates covered by the orbicularis muscle on the exterior surface. The ciliary margin in each is abrupt and thickened, causing the firmness of the edges of the eyelids. The orbital edge of each is thin, and attached to the base of the orbit by a fibrous expansion termed the broad ligaments of the tarsus. The object of these cartilages is to impart strength, pliancy, and elasticity to the palpebræ.
The Meibomian glands or follicles appear on the eversion of the palpebræ, as bony, pale, yellow, parallel ducts, leading from the free margin of each lid along the ocular surface of the cartilage, and covered by the mucous membrane; their openings are seen with a lens as a row of minute pores behind the cilia. They secrete an unctuous fluid which lubricates the edges of the lids and the cilia, prevents their friction and adhesion when closed, and hinders the overflow of tears when these are secreted in moderate quantity.
The conjunctiva, or internal integument of the palpehræ, lines these curtains, and connects them with the eye. At the free edge of each lid, it is continuous with the skin. Within the superior lid it ascends, and rises above the cartilage into a cul de sac, the superior palpebral sinus, which is loosely connected with the cellular and adipose tissue within the orbit, and is then reflected on the fore part of the sclerotic coat of the eye. It is continued over the cornea as an exceedingly delicate membrane, only separable by previous maceration. From the lower part of the sclerotic, the conjunctiva is reflected on the inner surface of the lower lid, forming the inferior palpebral sinus, and extends to the margin. At the inner canthus of the eye, it forms a vertical fold, the plica semilunaris. The caruncula lachrymalis is a small irregular eminence, placed in the lacus, at the inner canthus of the internal palpebral fissure, internal to the plica semilunaris. It contains a number of minute follicles, which secrete a sebaceous substance which often accumulates in the cornea.
3. Lachrymal Apparatus. This consists of the lachrymal gland and its excretory ducts, the two puncta lachrymalia, the lachrymal canals leading from each into the lachrymal sac, and lastly the nasal duct, leading from the latter into the nose.
The lachrymal gland is of a pale reddish color, surrounded by a cellular capsule, situated at the upper and outer aspect of the globe of the eye, a position from which its secretion can most eflfectually flow over the anterior surface of the globe. It consists of two lobes, a superior or orbital and an inferior or palpebral. Six or eight delicate ducts descend nearly parallel from the gland, and open opposite to its lower border by separate orifices on the inner surface of the upper lid, commencing about half an inch from the outer canthus, and a little above the upper margin of the cartilage. This organ secretes the tears which serve to lubricate the eye-ball, and to dilute the more viscid secretion of the mucous membrane. The lachrymal secretion consists of water, and about one per cent, of chloride of sodium (common salt), with a yellow extractive matter.
The puncta lachrymalia are the two small holes in the cartilaginous projections named lachrymal papillæ. They are always open and visible to the naked eye, at the inner extremity of the ciliary margin of each cartilage, and about two lines distant from the inner canthus. Each opening will admit a bristle. They are separated by the caruncula, and each leads into the following.
The lachrymal canals are two, a superior and an inferior. The superior ascends from the punctum, then bends downwards to the anterior and outer side of the sac. The lower canal just descends, then ascends and opens into the sac very near to the first.
The lachrymal sac is the upper extremity or oval cul de sac of the nasal duct, distinguished from it externally only by a small constriction, and internally by a semilunar fold. It is situated opposite to the middle meatus of the nose, receives the lachrymal secretions from the small ducts, and transmits them to the nose. It is usually filled with adhesive mucus.
The nasal duct leads obliquely downwards and outwards from the sac, and opens into the anterior part of the outer side of the roof of the lower meatus of the nose under cover of the inferior turbinated bone. It is about three fourths of an inch long, a little curved, and separated from the antrum by a thin but strong bony lamella. It is a fibro-mucous duct, inclosed in and rather loosely adherent to the bony canal, formed by the maxillary, unguis, and inferior spongy bones.
4. Muscles of the Eye. The orbit of the eye contains seven muscles, the interstices of which are filled with a quantity of soft adipose substance. These muscles are the levator palpebrse, four recti, and two oblique. All these except the inferior oblique arise near or around the apex of the cavity, and thence diverge to their respective insertions. These are situated above the optic nerve, the levator palpebrae, superior oblique, and superior rectus; two are beneath it, the inferior rectus and inferior oblique; and one is at either side, the internal and external rectus.
The levator palpehræ superioris is one of the largest and highest muscles in this region. It arises by radiated tendinous fibres from the upper or anterior border of the foramen opticum, and from the fibrous sheath of the optic nerve. It passes forwards in the axis of the orbit, becomes broad, thin, and fleshy, anteriorly bends downwards in front of the eye, and ends in a thin membranous expansion, which is inserted into the convex border of the superior tarsal cartilage, as also into the convexity of the superior palpebral sinus of the conjunctiva, behind or beneath the broad ligament of the tarsus. It serves to elevate the upper eyelid, also to retract its cartilage beneath the edge of the orbit. A branch of the third or motor nerve is distributed to it, which with the muscle when paralysed, permits the upper eyelid to droop downwards in front of the eye.
The remaining six muscles are proper to the eye-ball. Four are called straight, and two oblique. By their varied combinations, all the motions of the eye-ball are performed. The recti muscles are by no means straight, since all arise from the apex of the orbit, and diverging as they pass forwards, inclose a pyramidal space embracing the greater part of the globe of the eye, and bending a little around the fore part of the eye to reach their insertion. Each rectus muscle, then, represents a curve with its concavity towards the eye-ball. They are each of a triangular form, the apex behind, the base before. All terminate in front by thin tendons which extend to within a few lines of the circumference of the cornea. They are connected together by a cellulo-fibrous tissue named ocular fascia. The names assigned to the different recti muscles are rectus superior, or levator oculi; rectus internus, or adductor oculi; rectus inferior, or depressor oculi; and rectus externus, or abductor oculi.
The oblique muscles are two in number, the superior and the inferior. The obliquus superior or trochleator arises from the sheath of the optic nerve, and from the inner margin of the optic foramen. It passes forwards and ends in a round tendon, which passes through the cartilaginous pulley attached by a movable fibrous ligament to a depression behind the inner angle of the os frontis; the tendon then passes backwards and outwards, and is inserted into the posterior part of the sclerotic coat between the superior and external recti. In some instances the pulley is bony instead of cartilaginous.
The inferior oblique muscle is the shortest of the group, and the only one that is not connected to the apex of the cavity, being situated at the inferior and anterior part of the orbit, behind the lower eyelid. It arises from a rough ridge within the orbital margin of the superior maxillary bone external to the lachrymal sac, and ends in a broad thin tendon which ascends between the eye and the external rectus, becoming inserted into the posterior external part of the sclerotic. The two oblique muscles are adapted to rotate the eye on its axis. The recti muscles are adapted to change the position of the axis of the eye with reference to the axis of the orbit, and by the combination of the two sets of muscles, the axis of the eye can be turned with ease and precision to any object in front of the body.
5. Blood-vessels of the Orbit. The arteries are the ophthalmic artery and its ramifications, assisted by small vessels from the facial, temporal, and internal maxillary arteries. The ophthalmic artery, as the principal, arises from the internal carotid, just after the latter has emerged from the cavernous sinus, and is curving upwards by the side of the anterior clinoid process. It immediately becomes attached to the sheath of the optic nerve, and passing into the orbit, sends off numerous branches to supply the optic apparatus. The principal vein is the ophthalmic, which escapes from the orbit by the inner wide portion of the sphenoid fissure; it then enters the cavernous sinus, whence the blood is carried by the petrous sinuses to the internal jugular veins.
6. Nerves of the Eye. The nerves of the eye are large and numerous, no less than four entire nerves and a portion of three others being distributed to this organ. These nerves are the second, third, fourth, and sixth; one division of the fifth, and branches of the seventh or facial, and of the sympathetic. Each of the cerebral nerves arises from a distinct part of the nervous system, and ministers to some distinct and special purpose.
Pl. 131, fig. 1, well formed left eye of a middle-aged man, seen from the front: a b c, eye-brow; d, upper eye-lid; e r m, palpebral fissure; e f g h i, inner canthus of the eye, with the lacus and the lachrymal caruncle; k l, line showing the difference in height between the two canthi of the eye; m to q, lower eye-lid; r, outer canthus; s t v w, iris. Fig. 2, female eye, for comparison with the male. Fig. 39, lateral view of the eye. Fig. 3, left eye, as shown during a quiet sleep; a b c, eye-brow; odel, depressed upper eye-lid; e f, completely closed rima; g, lashes of both lids; h to o, translucent portion of the eye-lid; p, fold of the lower eye-lid. Fig. 4, eye-lids removed, and seen from behind: a, portion of the orbicularis muscle; b, rima palpebræ; c, lachrymal gland; d, its division into two lobes; e, excretory ducts of the lachrymal gland; f, their openings; g, conjunctiva; h, Meibomian glands; i, superior punctum lachrymale; k, Meibomian glands of the lower eye-lid; l, inferior punctum lachrymale; m, caruncle. Fig. 5, nearly the same view, but magnified: a, orbicularis muscle; b, rima; c, levator palpebræ; f, openings of the excretory ducts of the lachrymal glands; g, conjunctiva; h, Meibomian glands of the upper eye-lid; i, portion of the conjunctiva reflected, to lay bare the Meibomian glands; k, openings of these glands; l, glands of the lower eye-lid. Fig. 6, Meibomian glands, highly magnified. Fig. 7, inside of the eye-lids, with the puncta lachrymalia. Fig. 8, lachrymal apparatus: a b c d, upper and lower lachrymal canals; e f g, lachrymal sac; h i, nasal portion of the lachrymal sac; k l, lachrymal glands. Fig. 9, muscles of the left eye-ball: 1, 2, 3, outline of the orbit; 4, pulley for the tendon of the trochleator or superior oblique muscle; 5, eye-ball; 6, 7, optic nerve; a to e, levator palpebræ superioris; f g, superior, h i k, external rectus; l, inferior oblique; m, inferior rectus; n o, internal rectus; p to s, superior oblique muscle of the eye. Fig. 10, the same view, the levator palpebræ removed: 6, 7, optic nerve; g, superior rectus removed; h to o, the same as in the preceding figure; p to u, superior oblique muscle. Fig. 11 a b c, internal rectus; d e f, inferior, g h i, external rectus; k l m, inferior oblique muscle. Fig. 12, nerves belonging to the eye; 2 optic nerve; 3, third cerebral nerve or oculomotor; x, branch from it to the internal rectus muscle; 4, fourth cerebral nerve; a, branch from the fifth pair; 5, fifth cerebral nerve; a, central extremity; b, plexiform swelling; c, first branch; d, second do.; e, third do.; ff, foramen ovale; g, foramen rotundum; a, communicating branch between the fourth and fifth nerves; b to i, frontal branches; k to y, distribution of the lachrymal nerve; 6, 6′, 6″, sixth cerebral nerve. Fig. 13, ramifications of the third pair of nerves, and the ciliary ganglion: a, superior rectus muscle; b, b, levator palpebræ; 3, third cerebral nerve; a b, small upper branch; c, branch to the superior rectus; d, branch to the levator palpebræ; e, inferior branch; f, branch to the inferior rectus; g, lower branch; h, branch to the ophthalmic ganglion; ii, branches to the inferior oblique muscle; kkk lll m, branches proceeding from the ophthalmic ganglion (ciliary nerves); 5, fifth cerebral nerve; n, first branch; o p q r, four branches of the latter; t, branch to the nares; u, thread connecting it to the nerve of the superior rectus; v, branch to the ophthalmic ganglion; w, sixth cerebral nerve. Fig. 14, nerve of the inferior rectus muscle; branch from the fifth and sixth pairs to the nares: a, fifth cerebral nerve; b, Casserian ganglion; c, first, d, second, e, third branches of do; f, f, lesser portion; g, superior oblique muscle; b to v, the same as in the preceding figure; tz, inferior trochleator nerve; α, sixth cerebral nerve; ββ, branches of the sixth nerve to the carotid plexus; η, branch to the external rectus. Fig. 15, ramifications of the left ophthalmic artery: a to d, orbit; e, levator palpebræ, cut through and reflected; f g, superior rectus; h, internal rectus; k, external rectus; l, optic nerve; m, eye-ball; n o p, carotid artery; q r, ophthalmic artery; a b, ciliary arteries; c, artery to the lachrymal gland; d, ciliary branch of do.; e, feeble branch to the external rectus; f, branch to the inferior oblique muscle; f f, stronger branch to the external rectus muscle; g h i, separation of the lachrymal artery, and to the lachrymal gland and upper eye-lid. Fig. 16, veins of the eye: a b c, orbits; d e, eye-ball; f, optic nerve; g h, levator palpebræ; k, superior rectus; k, superior oblique muscles; l, pulley of do.; m n, external rectus, cut through; o, inferior rectus; a to m, branches to the facial vein; o p, ophthalmic vein; q r s, ophthalmic branch of the facial vein; t t, vein from the superior rectus; u u, superior ciliary vein; v v w w, lachrymal gland vein; x, posterior nasal vein; yy, veins from the sheath of the optic nerve.
The Eye-Ball
The ball or globe of the eye, or the eye proper, is placed at the anterior and internal part of the orbit, behind the conjunctiva, surrounded by fascia, muscles, vessels, nerves, and adipose substance, and retained in its situation by the optic nerve, the recti and superior oblique muscles, which support or suspend it in the surrounding fat, and admit of its free and easy motions. It is small in comparison with the cavity which contains it. In some persons it appears more prominent than in others; the variety in this respect depends partly on the amount of adeps in the orbit, and partly on the size of the palpebral opening; it is also absolutely larger in some than in others. The eye is nearly spherical, and about one inch in diameter, but, in consequence of the slight projection of the cornea, which is a segment of a smaller sphere superadded to the larger one formed by the sclerotic, the antero-posterior axis is one or two lines longer than the transverse. A transverse section, dividing it into an upper and lower half, or a vertical section, dividing it into a right and left portion, will exhibit an oval outline; but a perpendicular section, cutting it into an anterior and posterior half, will exhibit the circular form. The long axes of the eyes are nearly parallel to each other, and therefore not so to that of each orbit. The eye is a hollow globe, the wall or shell of which is composed of different membranes or tunics, and the cavity is filled by transparent fluids or humors for optical purposes. The coats are three, the sclerotic, the choroid, and the retina; these fit accurately one within the other, and are in close apposition. The first is called sclerotic; it is a fibrous membrane, for the protection and maintenance of the form of the organ; it invests the posterior four fifths, and presents a circular opening in front, into which the transparent cornea is inserted, which completes the anterior fifth; the cornea and fore part of the sclerotic are also covered by the conjunctiva. Within the sclerotic is the second tunic, the choroid, which is extremely vascular, and contains the nutrient vessels and nerves; it also secretes the brown or black pigment, which deeply stains the interior of the globe and the back of the iris, to prevent the reflection of the rays of light from the bottom and sides of the organ back again through the retina. In the anterior part of this tunic there is also a circular opening or deficiency, into which the iris is fitted, as the cornea is into the sclerotic. External to the circumference of the iris the choroid is intimately attached to the sclerotic by the ciliary band or ligament; and internally and behind the iris it is connected to the membrane of the vitreous humor by a series of folds, called ciliary processes, arranged in a circular form around the margin of the crystalline lens. The third, or innermost tunic, is the retina, the delicate expansion of the optic nerve; this extends from the entrance of the nerve, at the back of the eye, all around the interior of the choroid membrane, and terminates in front about two lines behind the anterior border of the latter; this is the essential part of the organ, being endowed with sensibility to light; all the other parts may be considered as subordinate to it. The humors of the eye are the aqueous, the crystalline lens, and the vitreous; these, though of different densities, and inclosed in membranous capsules, are all transparent, and exactly fill the globe. The aqueous fluid occupies the space between the cornea and the lens; the iris floats and moves in this fluid, and divides the space into two chambers, the anterior and posterior. The anterior is between the cornea and iris, and the posterior between the iris and the lens and vitreous humor; this space is very small, and both communicate freely through the pupil, or the circular aperture in the centre of the iris. All the posterior region of the eye is filled by the vitreous humor, a soft, gelatinous, transparent mass, composed of the most delicate cellular membrane, the cells filled with fluid. In a depression on the fore part of this substance, and behind the pupil and iris, is placed the crystalline fluid or humor, of greater density than either of the other two, and of the form of a double convex lens. We shall next proceed to the examination of these parts of the eye, in greater detail.
1. Tunica Sclerotica. This, together with the cornea in front, forms the external coat or case of the eye, and extends from the optic nerve to the circumference of the cornea; it is a dense, opake, fibrous membrane, very strong and inelastic, preserving the figure of the organ and protecting from injury and pressure the delicate structure within. Near the entrance of the optic nerve it is pierced by numerous small foramina, for the short ciliary nerves and vessels; more anteriorly, by small oblique canals for the long ciliary; and a little behind the transverse axis there are four or six larger canals for the exit of veins. The internal surface of the sclerotic is in contact with the choroid membrane, and is stained by the brown pigment. When washed clean it presents a smooth glossy appearance, owing partly to the presence of a very fine serous-like lamina. The thickness of the sclerotic is greatest posteriorly, about the optic nerve; thence it thins out towards the centre. The optic nerve perforates the sclerotic about a line and a half internal to the antero-posterior axis. As the nerve approaches this point, it is suddenly constricted; its fibrous sheath of dura mater is intimately united to the sclerotic, and the contracted nerve passes through a small aperture in the membrane which appears traversed by fibres, and has received the name of lamina cribrosa. When the nerve is squeezed, a central dark point will be observed in a section, called the porus opticus, and showing the position of the cerebral artery of the retina.
2. The Cornea forms the anterior fifth of the eyeball, and completes the external case, by joining on to the sclerotic; it projects beyond the level of the sclerotic, being the segment of a smaller sphere engrafted on the larger one formed by that membrane. It is perfectly smooth and transparent, circular in form, although the transverse diameter is slightly larger than the vertical. In man it is a concavo-convex lens of slight refracting power, owing to the fact of its greater thickness in the centre than at the edges. The margins of the sclerotic are bevelled off obliquely, the outer lamina extending further than the inner; between the edges there is a shallow groove, into which the cornea is fitted like a crystal in a watch. The cornea consists of several layers, some of these exceedingly delicate. Exteriorly there is a fine epithelial lamina, constituted by the prolongation of the conjunctiva. This becomes opake after death, causing the peculiar film over the eye. Next comes the cornea proper, consisting of transparent, soft, flexible laminæ, connected together by delicate areolar tissue. Posterior to the proper laminated cornea is a thin, strong, elastic, cartilaginous lamina, the membrane of Demours; it is perfectly transparent, and is placed between the cornea and the membrane of the aqueous humor. It extends beyond the proper cornea, and fits in by a well defined margin between the sclerotic and the ciliary ligament. The fourth layer of the cornea is the membrane or capsule of the aqueous humor, a tissue of exquisite delicacy.
The choroid coat is the second tunic of the eyeball, and is so named from an imaginary resemblance to the chorion of the gravid uterus. It is a soft membrane of a dark brown color, extending from the optic nerves as far forwards as the ciliary ligament, which is internal to the line of junction between the cornea and sclerotic, and external to the iris. This ligament and the iris may be considered as appendages to it. It is plexed posteriorly by an annular foramen for the passage of the optic nerve; anteriorly it presents a large opening for the iris. The choroid is extremely vascular and organized, and serves not only as a connecting medium between different parts of the organ, but also for conducting vessels and nerves to the interior, especially to the iris; it also secretes the dark pigment of the eye. This is deposited throughout its substance, more thickly, however, internally; the sclerotic is stained by it, but not the retina. This peculiar secretion is intended to darken the interior of the eye, as is done in the interior of optical instruments, to absorb the rays of light and to prevent their being reflected back again to the retina.
3. The Ciliary Ligament is a soft, spongy, fibro-cellular, annular band, of a greyish white color, not stained by pigment. It is continuous with the anterior margin of the choroid, internal to the line of junction between the cornea and sclerotic. The iris is inserted into its external border, and from its anterior aspect are continued the ciliary processes or folds of the choroid membrane. It thus serves as a common central medium to connect the various tissues of the eye.
4. Ciliary Processes, or corpus ciliare, are delicate folds or plaits of the choroid membrane, extending from within the ciliary ligament to the back part of the iris, and thence along the fore part of the vitreous humor to near the circumference of the crystalline lens; the entire series resembles the disk of a composite flower.
5. The Iris is the circular, vertical partition dividing the intervening space which contains the aqueous humor into two chambers, an anterior and a posterior, these communicating by the central circular aperture in the iris named the pupil. This opening is circular in the main, and a little nearer to the nasal than to the temporal side of the iris; its size varies with the distance of the object in view, the sensibility of the retina, and the intensity of the light. There is often a correspondence in color between the iris and the hair. The posterior surface is coated with a thick lamina of dark pigment named uvea, from a fancied resemblance to a ripe purple grape. The iris is highly organized, and receives its blood posteriorly from the long ciliary arteries, and anteriorly from the ophthalmic. The nerves of the iris are derived from the ophthalmic ganglion. The structure of the iris is pretty generally considered to be muscular, the exceedingly minute fibres being arranged in two series, one radiated, the other circular, concentric with the pupil. When enlargement is necessary, the sphincter or circular fibres relax, and the radiated acting from the circumference to the centre, approximate the inner margin of the iris to the outer, the reverse taking place when the aperture or pupil is to be diminished.
During the greater part of uterine life the pupil of the fœtus is closed by the membrana pupillaris, a delicate membrane filling up the aperture of the pupil, and completely separating the anterior from the posterior chamber. It actually consists of two thin laminæ, extending from the surface of the iris. It is most distinct about the fifth month, and becomes absorbed towards the period of birth.
6. The Retina is the third or innermost, or nervous tunic of the eye, and is in immediate contact with the vitreous humor which distends the posterior part of the globe. During life it is transparent, but soon becomes clouded. It is the expansion of the optic nerve into a membrane forming the portion of a sphere, and extending between the choroid and the vitreous humor to within about one eighth of an inch of the ciliary ligament. The optic nerve pierces the posterior part of the globe about a line and a half internal to the centre. About a line and a half to the inside of the entrance of the optic nerve, and in the part of the retina which would be pierced by the imaginary antero-posterior axis of the eye, there is a small circular or oval spot with a dark centre and a yellowish border. This has been called the foramen of Sæmmering or the punctum aureum.
The retina consists of three laminæ, each differing in texture and function. The exterior is the tunica serosa or Jacob’s membrane; it supports the nervous tissue and separates it from the pigmentary surface of the choroid. The internal is a vascular layer, composed of the capillary ramifications of the centralis artery and vein. The middle layer is the expanded medullary or fibrous substance of the optic nerve.
The cavity of the eye is occupied by refracting media, the humors differing from each other; these are the aqueous, the crystalline, and the vitreous, and are placed in this order between the cornea and the optic nerve.
7. The Aqueous Humor is a perfectly colorless liquid, occupying the interval between the cornea and the lens, and inclosed by a fine secreting membrane or capsule. It differs but little from water in specific gravity and refractive power. Chemically it consists of about ninety-eight parts of water and two of chloride of sodium, with a trace of albumen. The space occupied by this humor is divided into two apartments by the iris, anterior and posterior.
8. The Crystalline Lens is a transparent, double convex lens, the anterior convexity less than the posterior. The former forms part of a circle whose diameter is seven or eight lines in length, the latter one of four or five lines. Its convexity varies, however, with age. A perfectly transparent elastic capsule invests the lens proper. On opening the anterior part of the capsule of an eye long dead, a liquid escapes, known as liquor Morgagnii. This accumulation of liquid in all probability does not exist in the recent eye. The crystalline lens itself is of quite complicated structure. When boiled it can be separated into concentric layers, of which the exterior are soft, the internal increasing in hardness to the central nucleus. These laminæ appear to consist of parallel fibres united by finely serrated or toothed margins. During the separation of these laminæ, a moderate pressure will cause the whole to part into three triangular or wedge-shaped segments. In the recent lens, the density of the layers increases from the surface towards the centre, this involving a corresponding increase in refracting power. Consequently, rays of light falling on the exterior of the lens, will be refracted to the same focus as those passing through the centre meeting there a more highly refracting medium. Certain defects of vision depend greatly on abnormalities of the crystalline lens. Thus a convexity greater than usual produces short-sightedness by causing the rays of light to converge to a focus in front of the retina, thus necessitating an unusual approximation of an object to the eye. In long-sightedness, the lens being less convex than usual, the rays tend to a focus behind the retina, and to bring this point of convergence on the retina, the object has to be held at a greater distance.
9. The Vitreous Humor, or the Hyaloid Body, fills the posterior three fourths of the globe, and is in contact with the whole of the inner surface of the retina. Anteriorly and centrally the crystalline lens is imbedded in it, and more externally the ciliary processes are attached to it. In the adult it is perfectly transparent, and consists of a membranous capsule and areolar tissue secreting and inclosing a fluid like water. The hyaloid membrane or capsule not only incloses the humor, but sends inwards numerous processes, which join each other, and form a fine areolar or cellular tissue, in the interstices of which the fluid is confined. These cells all communicate with each other, as a single puncture will permit the gradual discharge of all the fluid. The vitreous body is traversed by a small artery from the centralis retinae, extending to the capsule of the lens. The vascular layer of the retina also in all probability sends into it vessels and nerves.
From the preceding description it must appear that the eye is not only of complete structure and delicate organization, but is also a refined optical instrument. The rays of light proceeding from any object strike upon the surface of the cornea, which being convex and much more dense than air, refracts them, and causes them to converge towards a distant focus. In passing through the anterior chamber, this convergence is slightly counteracted, and the degree of refraction is about equal to that which would have occurred had they impinged at once upon the convex surface of the aqueous humor, supposing the cornea not to have been interposed. Much of the light that traverses this fluid falls upon the iris, which, like the stop or diaphragm in any optical instrument, excludes it, and this light is reflected back again through the cornea. Hence we see the fibrous texture and variegated color of the iris when we look upon the eye of another. Those pencils of rays only which pass through the pupil are subservient to vision. As these pass through the lens they undergo two refractions, because this medium is convex on both surfaces, and is more dense than, either the aqueous or vitreous humor. These refractions increase the convergence of the rays, and bring them to their proper focus upon the sentient surface of the retina, on which is formed an accurate image of the various external objects from which the rays of light have been received. This image is inverted. What is above in the object is below in the image. The right side of the object is to the left, and the left to the right, while the relative position of its different parts remains the same. But as all surrounding objects, if seen, must be equally reversed, the relative position of all objects, therefore, remains unchanged, and there can be no comparison between what is erect and what is inverted, and, therefore, the sense acquires a correct idea of the position of objects. The fact, however, of our seeing objects erect, notwithstanding their images are inverted on the retina, as also that of single vision, from the simultaneous action of both eyes, and many other phenomena, has given rise to some interesting inquiries and to much speculation respecting the functions of the retina and optic nerves.
As the accurate convergence of all these pencils of rays to their respective foci upon the retina is necessary for the formation of a perfect image, and for clear and distinct division, certain nice adjustments in the apparatus are required, and have accordingly been supplied, and which in artificial optical instruments are attained with difficulty by mechanical skill. An image of an object, formed by a simple refracting medium, is liable to certain imperfections or aberrations of light. These are principally three, and are technically termed, first, aberration from sphericity; second, from parallax; and, third, chromatic aberration. Each of these we shall briefly explain, with a view of considering how they are obviated in the living eye.
Aberration from sphericity arises from this cause: a refracting spherical surface does not unite the parallel or diverging rays of a pencil exactly into one focus, because the lateral rays converge sooner than the central; hence arises a certain degree of confusion, which requires much attention to correct in the construction of the microscope or telescope. This correction is effected in the eye partly by the iris shutting off all circumferential rays, and partly by the form and texture of the lens. Its surfaces are not spherical, but elliptical, and it is more convex posteriorly than in front. Its density also increases from the surface to the centre, and, as the refractive power is proportioned to the density of the medium, so the rays which pass through and near the centre are brought to a focus sooner, and thus accord with those which are refracted more externally, and thereby that defect is obviated which occurs in lenses of uniform density.
Aberration from parallax may be thus explained. When the object viewed is very distant, the rays of light from it may be considered as nearly parallel; but, when the object is very near, the rays from it diverge considerably in their course to the eye. The effect of refraction on the distant or parallel rays is to bring them to a focus very near the lens; but the near or diverging rays are collected into their focus at a greater distance from it. The more remote the object, the nearer will the focus be to the lens, and for every distance of an object there is a corresponding focal distance behind the lens. If, therefore, the eye be adapted for vision at one particular distance, the images on the retina of objects at any other distance ought to be confused, because the foci will be formed either before or behind the retina. In the latter case this membrane will interrupt the rays in their course, and in the former it will not receive them until they have crossed each other in passing through their focus. This optical defect is counteracted by a power which the eye possesses, named adjustment, or accommodating itself to vision at different distances. The immediate agency in this power is not exactly ascertained, but most probably it depends on a vital energy of some of the textures in the globe. It has been ascribed by some to the fibres of the lens being muscular, and capable of altering its form, density, and distance from the retina; by others to a change in the convexity of the cornea, or to an alteration in the form of the globe by the compression of the surrounding muscles, or to a change in the position of the lens through the action of the iris and ciliary body, or through the contraction or erection of the ciliary processes.
Chromatic aberration depends upon the fact that rays of white light are composed of differently colored rays, red, orange, blue, &c., which are partly separated or dispersed by refracting media, and, as some colored rays are more refrangible than others, they will converge sooner; thus blue and violet are more refrangible than red or orange, and will sooner be brought to a focus, and thus the distinctness of the image will be impaired or confused, and fringed with different tints. This defect, which is termed chromatic aberration, is obviated in the eye by the employment of several refracting media, each of different density, and even of different chemical composition. Thus the lens has two unequally convex surfaces, each of which differs in density from its more central portions; the cornea and aqueous fluid form a refracting medium of different consistence from the lens or vitreous humor, and it is probable that the dispersive power of these may be disproportionate to their refracting effect, whereby an achromatic combination is established in the eye, as is effected in optical instruments, by combining lenses of different materials; we are not, however, to conclude that the eye is perfectly achromatic.
The two well known defects in vision, myopia and presbyopia, depend either upon some peculiarity in the refracting media, or upon a deficiency or weakness in the power of adjusting or accommodating the eye to vision at different distances. Myopia, or near-sightedness, may be caused by too great convexity of the cornea or lens, and is most common in early and middle life; the rays from a near object meet in their focus on the retina, and produce a distinct image; but the rays from a distant object, being nearly parallel, are more easily brought to a focus, and, therefore, meet before the retina, and only form undefined spectra upon it. The defect is partly corrected by means of a concave glass of suitable curvature; this causes the rays to become more divergent; therefore, they converge less quickly, and form their focus upon the retina. Presbyopia, or far-sightedness, is more common in old age, when the cornea and lens are less convex than in youth; the rays from distant objects, being nearly parallel, are refracted to a proper focus upon the retina; but those from near objects are not refracted soon enough, and, therefore, their forcus being formed behind the retina, they do not form the image upon the nerve. This defect is remedied by a convex glass, which will cause the convergence of the rays from a near object, and bring them more rapidly to a focus, so as to form the image upon the retina, instead of behind it.
Pl. 131, fig. 17, anterior half of a section of the eyeball: a, sclerotic coat; b, lamina fusca; c, choroid coat; d, pigmentum nigrum; e e f, retina; g h, ciliary processes; i k l, crystalline lens. Fig. 1[8], posterior half of the same eye: a–d, as in the preceding figure; e–k, retina; l, entrance of the optic nerve. Fig. 19, retina: b, foramen centrale; c, its yellow border; d e f, section of the optic nerve; g h i, three branches of the central vessels. Fig. 20, anterior view of the retina and of the vitreous humor: a b, retina; c d, corona ciliaris about the lens; c d, lens; d, foramen centrale; e e, blood-vessels of the retina. Fig. 21, exterior of the retina: b, foramen centrale; c d, optic nerve, e f g, corona ciliaris of the vitreous humor; h i, arteries. Fig. 22, choroid coat: a b, optic nerve; c–f, portion of the sclerotic; g–k, choroid coat; m, long ciliary artery; n, long ciliary nerve; o, long internal ciliary nerve; p p, long and short vessels of the choroid; q q, ciliary nerves; r, s, t, vasa vorticosa. Fig. 23, the same from the other side: a b, optic nerve; c–f, sclerotic; g h i, iris; m, vasa vorticosa; n p, ciliary nerves. Fig. 24, inner surface of the retina: a, foramen centrale; b b, folds of the retina; c, arteria centralis; c d e e, four branches of do. Fig. 25, the vessels of the retina magnified. Fig. 26, distribution of the vessels of the iris magnified: a b c, vasa vorticosa; f h, arteries of the iris; k k, their retiform distribution; m n, layer; l o, smaller circle of vessels. Fig. 27, nerves of the iris magnified: e b, branches of the ciliary nerves; b b, distribution on the border of the iris. Fig. 28, vessels of the iris and of the membrana pupillaris magnified. Fig. 29, lens of a newborn child in profile; fig. 30, lens of a child six years old; fig. 31, do. of a grown man; fig. 32, section of a lens preserved in alcohol to show its laminated structure; fig. 33, lens hardened by alcohol and split into several segments; fig. 34, exfoliated lens; fig. 35 a, three layers of a segment of a lens; fig. 35 b, an exfoliating lens magnified, showing its tendency to divide into three segments. Fig. 36 a b, iris, choroid, and pupillary membrane of a seven months’ fœtus with their vessels magnified: a b c, choroid; d e, membrana pupillaris; f g, long ciliary artery; 1 to 5, vasa vorticosa of the choroid. Fig. 37, the same figure nearly of natural size. Fig. 40, vertical section of the left eye, the eyelids closed. Fig. 41, do. the eyelids opened. Fig. 42, outline references to the two preceding figures: a–h, upper wall of the orbit; m–q, lower wall of do.; r–v, dura mater; w–z, forehead; a–d, eyebrows; e–w, upper eyelid; a–q, lower eyelid; 1 to 11, muscles of the eye; 12 to 18, optic nerve; 19 to 21, vessels and nerves of the eye; 22, 22, axis of the eyeball; 23, its largest transverse diameter; 28, centralis retinæ; 29, sclerotic coat; 30, pigmentum nigrum; 31 to 37, choroid coat; 38, 39, portion of the choroid uncovered by the retina; 36, 37, iris; 39 to 41, retina; 42 to 46, lens. Fig. 43, horizontal section of the two orbits and of one eye: α α β β, frontal sinuses; γ γ, fat in the orbits: a a b b, section of the ethmoid bone; c c, d d, e e, ethmoidal cells; g, sella turcica; h h, section of sphenoid bone; i i, sheath of the optic nerve; k k l l, section of the zygomatic bone; m m, section of frontal bone; r r, optic nerve; s, external, t, internal rectus muscle; u, eyeball of the right side; v, do. of the left in section; w w, sclerotic; x x, the choroid; y y, cornea; z z z z, coverings of the eye.
The remaining organ of sense, the tongue with its physiology, will be more conveniently examined in connexion with the alimentary canal We proceed next to the consideration of the organs of respiration and voice.
![]() Organs of Respiration and Voice
Organs of Respiration and Voice
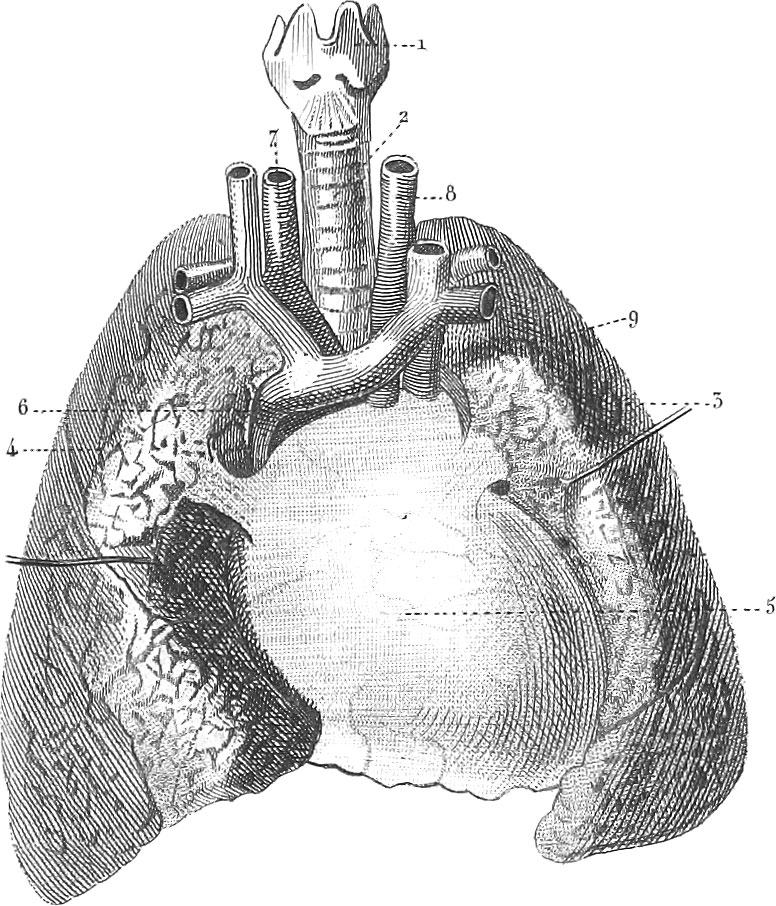 Organs of Respiration and Voice
Organs of Respiration and VoiceThe larynx, trachea, and lungs, constitute an apparatus, by means of which the oxygen of the atmosphere is introduced into the system and carbonic acid gas is exhaled. They are at the same time adapted to the production of sounds. We may even compare the lungs to the bellows of a musical instrument, the trachea to the air pipe, and the larynx to the tongue work.
The Larynx
The larynx surmounts the upper extremity of the respiratory passages, with which it communicates below as it does with the pharynx above; it is composed of a complicated apparatus of several cartilages, muscles, and ligaments, which constitute the organ of voice, and is suspended by muscles and ligaments from the os hyoides.
1. The Os Hyoides consists of five parts. The middle, or body, is concave posteriorly and convex anteriorly; on each side a cornu passes off, giving attachment to muscles above and below; and where each cornu joins the body, there is a small process called the appendix, which ascends obliquely backwards, and gives attachment to the stylo-hyoid muscle and ligament. When, as sometimes happens, this ligament is ossified, the os hyoides becomes attached directly to the cranium.
2. Cartilages of the Larynx, Four true or perfect, and four false or imperfect cartilages enter into the composition of the larynx. The former are the thyroid, cricoid, and two arytenoid; the latter are the two corpora euneiforma, and the appendices or cornicula of the arytenoid cartilages; there is also one fibro-cartilage, the epiglottis.
The thyroid cartilage is placed at the anterior and lateral parts of the larynx. It is composed of two broad lateral plates, connected in an anterior median prominence, known as the pomum Adami or Adam’s apple, and larger in the male than in the female. The posterior surface of the pomum gives attachment to the ligament of the epiglottis and to the chordæ vocales.
The cricoid, or annular cartilage, forms the lower part of the larynx. The inferior edge is nearly circular and horizontal, and gives attachment to the first ring of the trachea; the superior margin is oblique, and separated from the thyroid cartilage by the crico-thyroid ligament.
The arytenoid cartilages are situated vertically on the articulating surfaces on the upper and posterior border of the cricoid. The base of each presents two processes, one for the attachment of the crico-arytenoid muscle, the other for the insertion of the inferior chorda vocalis. The apex of each arytenoid inclines a little backwards, and is surmounted by the appendix, or corniculum. The internal or opposed sides of the arytenoid cartilages are smooth, and covered by mucous membrane, so as to admit of their approximation.
The epiglottis stands behind the base of the tongue, nearly erect in front of the opening of the glottis, over which it can be bent almost horizontally, so as to cover this opening during deglutition. In form it is somewhat triangular or oval, so as to resemble a cordate leaf, with the edges slightly curled.
The larynx is articulated or connected to the os hyoides by three hyothyroid ligaments, one middle and two lateral. The thyro-arytenoid ligaments, or chordæ vocales, are four in number, two on each side, a superior and an inferior. The ligaments of the epiglottis are the thyro-epiglottidean, the hyo-epighttidean, and the frænum epiglottidis. This latter, however, is only a fold of mucous membrane, connecting the epiglottis with the tongue.
3. Muscles of the Larynx. The muscles of the larynx are symmetrical; they are found on the front, sides, and back part. Those on the fore part are the thyro-hyoid and crico-thyroid; those on each side are the thyro and lateral crico-arytenoid; the muscles of the back part are the arytenoid and the posterior crico-arytenoid.
The openings of the larynx are two, the superior or the glottis, and the inferior or the tracheal. The superior opening, or the glottis, is at the lower and anterior part of the pharynx, behind the epiglottis and rather beneath the tongue. It is of a triangular form, the base anteriorly formed by the epiglottis: the sides are composed of the aryteno-epiglottidean folds of mucous membrane; and the apex, which is posteriorly notched or bifid, is formed by the appendices of the arytenoid cartilages. The inferior opening of the larynx is always free, and nearly a perfect circle, formed by the lower border of the cricoid cartilage, which is connected to and continuous with the trachea.
Intermediate between these two openings, and nearly midway within the larynx, is a very remarkable slit-like narrowing of its cavity, named the rima glottidis. This, the seat of the vocal function, is bounded laterally by the chordæ vocales. Its form is variable, and depends on muscular action, being subject to change in shape and size during every act of respiration, voice, and speech. Immediately above the true chordæ vocales, the larynx presents on each side a lateral dilatation, called the ventricle or sinus of the larynx. This space is bounded by the semilunar folds known as the false or superior chordæ vocales. From each ventricle the mucous membrane is prolonged upwards in a thimble-like form, constituting a pouch, the sacculus laryngis.
The arteries which supply the larynx are derived from the superior and inferior thyroid, the former a branch of the external carotid, the latter of the subclavian. The laryngeal nerves are four in number, a superior and an inferior on each side.
Pl. 129, fig. 32, thyroid cartilage; fig. 33, cricoid do.; fig. 34, arytenoid do.; fig. 35, epiglottis; fig. 36, section of the larynx: 1, upper, 2, lower vocal cord; 3, ventricle. Fig. 37, larynx from before: 1, os hyoides; 2, ligament connecting the os hyoides with the thyroid cartilage; 3, thyroid cartilage; 4, ligament between the thyroid and the cricoid cartilage; 5, cricoid cartilage. Fig. 38, larynx from behind: 1, glottis and epiglottis; 2, 3, ventricles.
Pl. 127, fig. 57, transverse and oblique arytenoid muscles. Fig. 8, larynx from the left side, one half of the thyroid cartilage removed: 1, posterior crico-arytenoid muscle; 2, lateral do.; 3, thyro-arytenoid muscle; 4, muscles of the epiglottis.
The Trachea
The trachea, continuous inferiorly with the larynx, is a tube composed of from sixteen to twenty-six C-shaped cartilaginous rings, open posteriorly. It commences opposite to the fifth cervical vertebra, and descends to about the third dorsal, where it divides into two branches, called bronchi, one of which passes to each lung, and there again subdivides. The right bronchus, shorter and broader, extends for an inch before it divides into three branches. The left bronchus, about an inch longer, sinks into the lung on the left side, below the corresponding pulmonary artery, and opposite the fifth dorsal vertebra. The cartilaginous rings determine the shape and diameter of the trachea, but do not lie in immediate contact, being separated and connected by elastic fibrous ligaments, by which the elongation and contraction of the tube are rendered possible. The posterior portion of the trachea corresponding to the gaps in the cartilaginous rings, is occupied by a layer of long yellow elastic fibre, a transverse muscular layer, and a mucous layer consisting of basement membrane and epithelium. This posterior soft portion, in immediate contact with the anterior of the œsophagus, readily yields to the pressure of the food passing down the latter tube. The entire length of the trachea amounts to about four or five inches, and on the exterior circumference of the bronchi are seen numerous lymphatic glands filled with a black pigment, and called glandulæ bronchiales.
Pl. 129, fig. 37, trachea and its branches from before: 6, trachea; 7, 8, cartilaginous rings; 9, yellow elastic fibres; 10, right, 11, left bronchus, with their ramifications. Fig. 38, posterior view of the trachea: 4, yellow elastic fibres, with their glandular granules; 5, muscular layer, composed of transverse fibres; 6, 7, soft elastic longitudinal fibres, strengthening the mucous membrane, 8.
The Lungs
The lungs, pulmones, constitute two conical spongy and elastic bags, occupying, with the heart between them, the cavity of the thorax. The color of the lungs varies, in different parts and at different times, between bright red and dark purple. Their weight amounts in the male to about two and a half pounds, in the female to about two pounds. Each lung forms a cone, with the broad base resting on the diaphragm, the apex being directed upwards. On the inner opposed faces of each lung is a shallow depression into which the bronchi and vessels enter and emerge. The right lung is divided by a fissure, nearly two inches deep, into three, and the left into two lobes. Each lobe exhibits externally a great number of small angular spaces, bounded by darker lines. Each bronchus, on reaching the lungs, divides into as many branches as there are lobes, and these, entering the lobes, subdivide and bifurcate again and again, until the exceedingly minute ramifications end in small air cells, which in the adult probably communicate with each other. On inflating the lungs, these cells will become dilated, and project on the surface in small mammillary or botryoidal swellings. The bronchi, as they penetrate into the lungs, gradually lose their cartilaginous element, until finally they consist of a soft membranous tube, which ends in the cells above referred to, the number of which has been estimated at seventeen or eighteen hundred millions.
The pulmonary artery, which conducts venous blood from the right ventricle of the heart, follows all the ramifications of the bronchi, and on the air-cells breaks up into a very delicate vascular plexus, from which the pulmonary veins take their origin. The venous blood circulating through this network of vessels absorbs oxygen from the air with which it is brought into contact by means of the air vessels. It then changes color, giving up a portion of carbonic acid and water. This change effected, it returns through four veins, two for each lung, to the left auricle. These vessels have nothing to do with the nourishment of the lungs themselves, this office being performed by the small broncbial arteries which proceed directly from the aorta, and from independent plexuses in the lungs which yet communicate with those of the pulmonary artery. The returning bronchial veins, too, lead partly to the superior vena cava and partly to the pulmonary veins, so that there is always a small quantity of black blood mixed with the arterial in the left auricle. The nerves destined to the lungs proceed from the vagus and sympathetic. The lungs have comparatively little sensibility, as even in extensive pulmonary diseases but little pain is felt.
Pl. 130, fig. 4, larynx, trachea, pericardium, and lungs, from before: 1, larynx; 2, trachea; 3, 4, lungs; 5, pericardium; 6, superior vena cava; 7, arteria innominata; 8, left carotid artery; 9, left subclavian artery.
The organs contained within the thoracic cavity are inclosed by three completely closed serous sacs, the two pleuræ and the pericardium. The latter has already been described with the heart. Each pleura is a short sac of a conical shape, and contains only the serous vapor it exhales; although the lung appears within the cavity, it is really external to it or behind it. That portion of each which invests the lungs is called pleura pulmonalis, that connected with the parietes of the thorax being the pleura costalis or parietalis. The relations of the lungs to the pleura may be better understood by supposing the latter at first to occupy the thorax exclusively. They will then constitute two bags, in contact with each other by their inner and opposed faces. If now the lungs are considered to be developed on the outside of the opposed surfaces of each bag, they will force this out towards the exterior, and finally connect each bag into two contiguous laminæ in contact with each other, the one the costal and the other the pulmonary pleura. The small space left anteriorly and posterior to the sternum is called the anterior mediastinum; that posterior and in front of the vertebræ is the posterior mediastinum. The space between the two, the middle mediastinum, contains the lungs and heart. The anterior mediastinum is wider superiorly and inferiorly than in the centre, and is somewhat X-shaped; the superior portion contains the origin of the sterno-hyoid and thyroid muscles, and the remains of the thymus gland. The posterior mediastinum is longer than the anterior, and includes the œsophagus, the larger blood-vessels, and the thoracic duct.
Pl. 130, fig. 3, cross-section of the thorax to exhibit the course of the pleuræ: 1, heart within its pericardium; 2, 3, substance of the lungs; 4, right pleura arising from the ribs and their cartilages; it bends back along the sternum, leaves the anterior mediastinum, 5, between it and the left pleura, passes over the pericardium, embraces the pulmonary vessels, passes over the lung, bends back again posteriorly, 7, the posterior mediastinum being formed between it and the left pleura as before.
1. The Thyroid Body or Gland is a large, soft, red mass, of a crescentic shape, and lying on the trachea and sides of the larynx. It consists of two large pyramidal portions, called lateral lobes, connected by a narrow slip, the middle lobe or isthmus. The thyroid body is surrounded by a fine tissue; it is of a soft spongy texture, the cells containing a yellow fluid. Four arteries, two from the carotid and two from the subclavian, are distributed to it. Its proper function is not known, although some consider it to belong to the secreting glands, while others with more probability suppose it to be in some way concerned in sanguification. It is very subject to enlargement by disease, constituting the affection called bronchocele or goitre.
2. The Thymus Body is another organ of ambiguous character, and only in its highest state of development in the fœtus before birth. It occupies the greater portion of the anterior mediastinum, and after birth decreases, until by the time an individual arrives at puberty it will have almost entirely disappeared. Some authors suppose its function to consist in the preparation of a fluid, like chyle, and fitted for fœtal growth before birth, and before chyle can be formed from food.
The Function of Respiration
The process of breathing consists of two distinct operations: inspiration, by which the external atmospheric air is brought into contact with the blood and yields up oxygen, and expiration, in which the carbonic acid formed in the combustion of the oxygen is exhaled together with other gaseous matters. The chemistry of breathing is a consequence of these physical operations.
Inspiration, or the drawing in of the breath, is produced by the expansion of the thorax, by which a partial vacuum being effected, the air rushes into the lungs and inflates them. A subsequent contraction of the parietes of the thorax will cause the expulsion of the air thus introduced. The glottis is connected with the pharynx, from which there are two ways for the air to escape or enter, one through the nostrils, the other through the mouth. It is more usual, however, when not otherwise influenced, to inspire through the former and expire through the latter. At the instant of inspiration, the thorax enlarges in all its dimensions; the diaphragm is depressed or drawn down, the ribs are raised and drawn outwards, this involving a protrusion of the sternum. In expiration all parts return to their former position. The muscles especially concerned in respiration are, the diaphragm, the intercostals, the levatores costarum, the scaleni, the serrati, the sterno-cleido-mastoid, longissimus dorsi, and the subclavius. The abdominal muscles are chiefly employed in expiration, but are assisted by the quadratus lumborum and the triangularis sterni. There are, however, other muscles concerned in respiration, especially such as fix the head, neck, and back, for the better action of the first set. In children, the abdominal muscles are more especially called into requisition, as shown in the rise and fall of the abdomen in breathing. In adult males this rise and fall are seen in the lower part of the thorax, while in women it is the upper part of the chest that heaves.
The entrance and escape of air are accompanied by a peculiar sound, distinctly audible by applying a stethoscope to the chest. The normal sound thus observed varies materially in diseases of the lungs and air passages, so that this instrument gives invaluable indications as to the extent and nature of pulmonary disease.
Physical and chemical phenomena of respiration. The tension of the gases in the air passages of the lungs varies according to the intensity of respiration. In quiet breathing, this amounts to \(\frac{1}{30}\) or \(\frac{1}{40}\) of the strength with which the blood usually flows in the larger arteries. In feeble respiration the amount is not more than half of this. These values increase with any obstruction to respiration. The circumference of the thorax at the pit of the stomach in full grown men, amounts during quiet respiration to from \(\frac{11}{25}\) to \(\frac{1}{2}\), rarely \(\frac{1}{20}\) of the length of the body. Each single aspiration continues longer than a contraction of the heart, and its duration increases with age. The new born infant generally respires forty-four times in a minute, the child of five years only twenty-six. From fifteen to twenty years, twenty times; from twenty to twenty-five, eighteen times; from twenty-five to fifty, sixteen or eighteen times. A mean act of respiration, therefore, in the adult lasts from three to four seconds. These values are of course subject to considerable variation.
The air introduced into the lungs is first brought to the temperature of the body, whatever be the temperature of the external atmosphere. Again, the air in the lungs is saturated with moisture, the amount dependent upon the barometric pressure and the temperature. During respiration in a cool atmosphere, the exhaled air must contain more moisture than the atmosphere itself Consequently the blood loses more moisture in winter than in summer, this difference, however, being equated by the greater loss by perspiration during the latter season; in winter again, the amount of urine discharged is greater. The amount of water lost depends upon the size of the lungs. Adult men between seventeen and thirty-five years may lose from \(\frac{1}{2}\) to \(\frac{18}{25}\) pounds in twenty-four hours. The number of aspirations does not seem materially to affect the result.
The composition of atmospheric air is pretty much the same in all countries and during each season of the year, the variation observed being exceedingly slight. Recent experiments show that there are 20.81 parts of oxygen and 79.19 of nitrogen by volume, and 22.01 of oxygen and 76.99 of nitrogen by weight. The amount of carbonic acid appears subject to decided variation, although, under ordinary circumstances, it is exceedingly slight. The air over the sea appears to contain less oxygen than that above the land and along the coast; and again, on the other hand, the air (contained in snow is richer in this gas. According to some observers, the amount of oxygen in the air of high mountains and deep mines is less than the standard.
A series of carefully conducted analyses of expired air shows that the oxygen is in much less proportion than in the atmosphere, while there is a large amount of carbonic acid. This carbonic acid must therefore have been formed in the system by the combination of oxygen with carbon of the blood. The amount of oxygen absorbed is about 23 per cent. The total amount of carbonic acid exhaled by a man within a given time may be expressed either by weight or volume, or by the value of the carbon contained in it. 275 parts by weight of carbonic acid contain 75 parts of carbon and 200 of oxygen. In one hour 10.572 grammes of oxygen are consumed, that is. 38.764. grammes of carbonic acid are generated. This amount varies greatly, however, with age, sex, and external conditions.
In males the carbonic acid exhaled regularly increases from eight to thirty years of age; from thirty to forty it is stationary; and from fifty to extreme age it goes on diminishing. It is greater in males than in females at all ages beyond eight years. In females, nearly the same proportionate increase goes on to the time of puberty, when the quantity abruptly ceases to increase, and remains stationary as long as menstruation continues, again to increase when this ceases. The more robust the individual, the greater is the amount of carbonic acid given off.
Although the volume of the nitrogen taken into the lungs remains nearly the same, yet there is a constant absorption and exhalation of this gas. The amount is somewhat greater in summer than in winter. There is usually some organic matter contained in exhaled air, either chemically or mechanically, as sulphuric acid is reddened by being breathed through for a considerable time.
The reaction which takes place between the air and the blood is one of simple endosmose and exosmose. If the blood come to the lungs charged with carbonic acid, and is exposed in their cells to the influence of atmospheric air, which is a mixture of oxygen and nitrogen, the carbonic acid will pass out, to be replaced by oxygen and nitrogen. The quantity of oxygen which enters will be much greater than that of nitrogen, owing to the superior facility with which oxygen passes through porous membranes. If the venous blood contain nitrogen as well as carbonic acid, it also will pass out, to be replaced by oxygen. The relative amount of these several interchanges of gases will be subject to continued variation from secondary causes. The combination of oxygen with carbon, to form carbonic acid, takes place not only in the lungs, but throughout the whole system, and this combustion is attended with the evolution of a considerable amount of heat. To this is mainly to be ascribed the animal heat of the body, which in man amounts at a mean to about 100° F.
![]() Organs of Digestion (Splanchnology)
Organs of Digestion (Splanchnology)
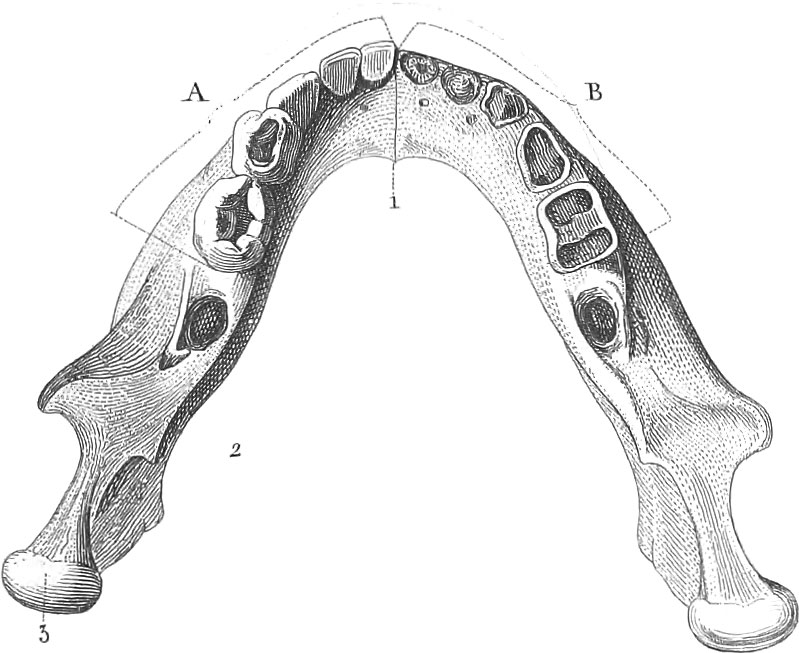 Organs of Digestion (Splanchnology)
Organs of Digestion (Splanchnology)The daily wear and tear of life, involving the destruction of life in individual atoms of the body, the loss of matter in the secretions and excretions, and the necessity of supplying fuel to keep up the temperature of the body, all require the constant introduction of fresh organic matter to supply the waste. A wise Providence has imparted to us certain sensations, known as hunger and thirst, by means of which we are enabled to ascertain when solid and liquid food is required. The various alimentary substances are taken into the mouth and masticated by the teeth, then carried to the stomach after having been mixed with the salivary secretion. In the stomach, the food is acted on by the gastric juice, and reduced to a pulpy mass termed chyme. Passing out of the pyloric orifice, the chyme enters the small intestines, and after having been mixed with the juices secreted by the pancreas and liver, becomes converted into chyle, and a residuum. The former is taken up by the lacteals, and ultimately poured into the descending current of venous blood; the latter passes in the form of excrement. Such are the general changes which take place, to be more fully described hereafter.
Such substances are alone adapted for purposes of nutrition as contain water, and a greater or less amount of organic matters capable of mixing with the fluids of the body. Certain nations, indeed, forced by custom or by necessity, devour mineral matters, as the Otomacs and Guamos in Guinea, who eat a clay, the inhabitants of New Caledonia, who mix a certain earth with their food, and the Laplanders, who in time of scarcity consume the bergmehl, tripoli, &c.; but these contain a small amount of organic matter, being composed almost entirely of the shields of infusoria. A long continued use of these substances is, however, exceedingly pernicious. Proper food must contain organic matter in a form capable of being assimilated by the digestive organs, and must include all the elements of the body. For this reason, starch and sugar cannot alone sustain life for a great length of time, owing to the absence of the necessary nitrogen, sulphur, phosphorus, and lime; and some substances even which fulfil these conditions may be incapable of supporting life. Thus, the fibrine of the blood contains most of the necessary elements, yet a dog fed exclusively upon it soon dies. The same applies to the gelatine from boiled cartilage and bones, tendons and ligaments. A well regulated alternation in the character of food consumed is imperatively required by the system. Thus the coagulated white of egg, when mixed with other substances, is exceedingly nutritious, yet animals cannot live upon it exclusively for any great length of time without danger to life. The same principle holds good in respect of the exclusive use of meat or of any other food.
The organs of digestion consist of an uninterrupted alimentary canal extending from the lips to the anus, and of numerous glandular bodies placed along its track, and pouring into it their secretions. This canal is in three portions, a superior, middle, and inferior, constituted by, first, the mouth, pharynx, and œsophagus; second, the stomach and small intestines; and third, the large intestine. The glandular organs are the salivary glands, the pancreas, the liver, and the spleen.
Organs of Mastication and Deglutition
1. The Mouth. The mouth, or cavum ori, is bounded anteriorly by the lips, superiorly by the hard and soft palate, laterally by the cheeks, inferiorly by the tongue and mucous membrane reflected from it to the gums; posteriorly it communicates with the pharynx; this opening is named the isthmus faucium, is bounded above by the velum and uvula, below by the tongue, on each side by the arches of the palate.
The anterior part of the palate, or hard palate, is formed of the palate plates of the maxillary and palate bones, covered by mucous membrane and glands; the posterior part of the palate, or soft palate, or velum pendulum, consists of a dense aponeurosis, and of several muscles and glands, inclosed in mucous membrane.
The cheeks are formed of mucous membrane, covered by the buccinator and a quantity of fat; several small mucous glands lie between the membrane and this muscle, and towards the upper and back part on each side we perceive the small opening of Steno’s duct.
The lips are composed of integuments with more or less of fat, muscles, vessels, nerves, glands, and mucous membrane. The skin is delicate and vascular, particularly at the red borders, where it is continuous with the mucous membrane of the mouth. The cuticle is continued over the latter to line the whole cavity as a very fine epithelium. The muscles are, the orbicularis oris, with which the fibres of many others (already described) intermingle. The arteries of the lips are the coronary vessels, assisted by their inosculations with branches of the internal maxillary artery. The sentient nerves are derived from the infra-orbital and dental branches of the fifth, and the motor from the seventh pair. The labial glands are very numerous; they are rounded and pale, and are situated in the submucous, loose cellular tissue, at some distance from the red border. The mucous membrane is continued from each lip to the alveolar processes of the maxillæ, and forms in the centre of each a small fold or frænum; this is larger in the upper than in the lower lip.
The mouth is lined throughout by mucous membrane, which is continuous with the cutis on the lips, and extends posteriorly through the pharynx, whence it ascends to line the nares, the Eustachian tube, and tympanum, on each side, and descends to line the œsophagus and larynx; it is also continued into the ducts of the sublingual, submaxillary, and parotid glands; as it is reflected from one surface to another, it forms folds or fræna, as between the lips and alveoli and beneath the tongue; at the sides of the fauces, also, it forms two semilunar folds on each side, called the pillars or arches of the palate; these folds inclose muscular fibres, which we shall examine afterwards.
On looking into the mouth, either in the living or dead subject, the following objects strike the attention: inferiorly, the tongue and inferior teeth; laterally, the cheeks; posteriorly, the back part of the pharynx; superiorly, the superior teeth, the hard and soft palate, from the centre of the latter the uvula, and from the sides, the pillars or arches descending to the tongue and pharynx; in the recess between these pillars on each side, the tonsils or amygdala are also seen; lastly, if the tongue be drawn forward, the epiglottis comes into view.
Pl. 129, fig. 30, cavity of the mouth: 1, palate; 2, velum palati; 3, uvula; 4, arch of the palate to the mucous membrane of the pharynx; 5, arch to the tongue; 6, tonsil; 7, tongue; 8, epiglottis, and beneath this the pharynx opened. Fig. 31, pharynx opened from behind, showing the posterior part of the fauces: 1, internal pterygoid muscle; 2, stylo-pharyngeal muscle; 3, 4, posterior nares; 5, velum palati with the uvula; 6, 7, its two crura to the tongue; between them the depression for the tonsils, 8; 9, isthmus faucium; 10, base of the tongue; 11, opening of the larynx; 12, posterior wall of the larynx; 13, portion of the trachea.
2. The Tongue, though somewhat triangular, is of a very variable shape; its base, thick and broad, is connected to the epiglottis and to the palate by folds of mucous membrane (the former are the fræna of the epiglottis, the latter are the arches of the palate), and to the os hyoides and inferior maxilla by muscles, to the latter also by a mucous fold, the frænum linguæ; the apex is thin and unattached; that portion between it and the base is named the body of the tongue; all the upper surface, the sides, and about one third of its inferior surface, are covered by mucous membrane, which is very rough superiorly, from the number of papillæ that project through it; anteriorly, these papillæ are small, conical, and connected with the terminations of the nerves of taste; posteriorly they are large, round, fungiform, lenticular, and very irregular; these are small glands which open on the mucous surface; near the epiglottis these glandular papillæ are often observed to have a peculiar arrangement, like the letter V, the concavity turned forwards; these are of a conical form, the apex attached in a little membranous cup or calyx; behind the apex of this angle a deep depression (foramen cœcum) is observable; this contains some mucous follicles. A superficial groove or raphe runs along the dorsum or top of the tongue; one more distinct exists along the inferior surface; and a cellulo-ligamentous line divides it mesially into two symmetrical portions. This line is more distinct near the base; in some animals it is very dense and even bony; in paralysis one side only of this organ is frequently found affected. The substance of the tongue is composed of adeps blended with numerous muscular fibres derived from the stylo, hyo, genio-hyo-glossi, and lingualis muscles, and of many other fleshy fibres which do not properly belong to any of these; two large arteries (lingual) and six considerable nerves (the gustatory, the lingual and the glosso-pharyngeal, on each side) supply this organ. The tongue is not only the organ of taste, but by its great mobility it assists in speech, in suction, and in deglutition. The fifth pair of nerves endow the tongue with sensation and with the sense of taste, the ninth with mobility, and the eighth supply its base with sensation, and connect the motions of this organ with those of the pharynx and stomach.
Pl. 129, fig. 27, dorsum or top of the tongue: 1, foramen cœcum; 2, 2, fungiform papillæ of the tongue; 3, 3, 3, 3, conical papillæ; 4, 4, 4, 4, series of filiform papillæ; 5, mucous gland of the base of the tongue; 6, 6, 6, folds of the mucous membrane to the epiglottis.
Pl. 127, fig. 4, hyoid muscles of the right side: 1, anterior; 2, posterior belly of the digastric muscle; 3, mylo-hyoid muscle; 4, stylo-hyoid do.; 5, stylo-glossus muscle; 6, stylo-pharyngeal do.; 7, sterno-hyoid do.; 8, omohyoid muscle; 9, thyro-hyoid muscle; 10, sterno-hyoid muscle. Fig. 7, muscles of the tongue: 1, stylo-glossus; 2, hyo-glossus; 3, lingualis; 4, lower end of the genio-glossus; 5, its anterior, and 6, its posterior fasciculus; 7, median line of the tongue.
3. The Teeth. The teeth are small, hard bones, thirty-two in number in the adult, sixteen in each jaw; their form is generally conical, the apex in the alveoli. In each tooth we distinguish the crown, neck, and root. The crown is external to the alveolus; it has no periosteum, but is covered by a firm, white, vitreous substance, named enamel. The neck is surrounded by the gum, and the root is firmly held in the alveolus by a mode of connexion called gomphosis; it is covered by the periosteum which lines the alveolus, and which is reflected upon it from the point to the neck. The root or fang of each tooth is perforated by a small hole for the nutrient nerve and vessels. The teeth are divided into three classes, the incisores, the canini, and the molares.
The incisores are four in each jaw. The crown of these is sharp and wedge-shaped, convex before, and thickly covered with enamel. The neck is constricted, and the root is conical, but flattened on each side. Those in the upper are stronger and larger than those in the lower jaw; the former are broader; their edge is like a chisel, cut off posteriorly; the latter are more vertical, and bevelled off anteriorly; they are not so sharp as those in the upper jaw; their roots are larger. The middle incisors in the upper jaw are much larger than the lateral, but in the lower the lateral are a little larger than the middle.
The canine teeth, or cuspidati, are two in each jaw, or one on each side of the lateral incisors. The crown is conical, a little blunt, convex before; their root is single, but very long, and larger than those of the incisors, flattened at the side, and grooved. Their alveoli are often very prominent.
The grinders, or molares, are twenty in number, ten in each jaw. The crown of these is broad and irregular; the roots are more or less divided. The two first molars on each side in each jaw are called bicuspidati, and are of an intermediate size between the canine and posterior molars. They have only two tubercles on the crown, which is rather round. The fangs in some are single, but usually double; the lower are smaller than the upper, and the tubercles on the crowns are not so deeply separated. The first lower bicuspid frequently wants the inner tubercle, and resembles a canine. The posterior grinders are the true molars or multicuspidati, three on each side in each jaw. These are large; the crown is somewhat square, has four, and sometimes five tubercles; the neck is thick and round; the root has three or four divisions, and each is perforated by a small hole. The crowns of the lower are rather larger than those of the upper; the latter are vertical, but the former are inclined a little inwards. The fangs of the lower are usually two, but very broad and strong, placed anteriorly and posteriorly, often much curved, flattened before and behind, grooved and often bifid. The first and second upper have usually three roots, one internal, two external; sometimes they have four. The first molar is generally the largest; the last, or dens sapientioe, is the smallest; its crown is short, and has only three tubercles, two external and one internal. The root, though often single, is grooved, and sometimes presents three partial divisions in the upper and two in the lower. These last teeth, however, are very variable as to size and other characters, and occasionlly are not protruded, particularly in the upper jaw.
Every tooth, when divided, presents an external shell or cortex, and an internal cavity which extends beneath the crown, partly corresponding to it in form, and contracts as it descends through the root into a fine tube, which ends in a minute foramen. In the young and growing tooth this cavity is large, and contains a soft, vascular pulp or bulb; in the course of time it is much diminished by surrounding osseous or ivory deposit, and in the adult or aged contains little more than a vascular lining membrane. The walls of this cavity, though very firm, are perforated by numerous minute pores, which lead into the solid texture of the tooth. The substance of a tooth consists of three elements: enamel, ivory or dentine, and crusta petrosa or cement. The enamel covers the crown; the ivory forms the greater portion of the body and root; and the crusta, in the form of a thin lamina, invests the root only, though, according to some, it is also prolonged over the crown and enamel.
The teeth make their appearance at a very early age of the fœtus, although requiring a long time for their full development; it is not till the sixth or seventh month after birth that the two middle incisors of the lower jaw come out. The remaining incisors follow at intervals of from four to six weeks; first the two median upper ones; then the two exterior lower, and lastly the two exterior upper. The upper and lower anterior molars of each side of the jaw next make their appearance, followed by the canines, and finally by the posterior molars. At the end of the second year the child has twenty teeth. These are called milk teeth, from making their appearance during the period of suckling. The incisive and canine milk teeth are smaller than the permanent; the posterior molars on the other hand are larger. About the seventh year the milk teeth fall out and are replaced by the permanent, in nearly the same order as that of their first appearance. After all the incisors are changed, the anterior and posterior temporary molars are successively shed, and replaced by the permanent bicuspids; the canines are not changed before the tenth or eleventh year. After the twelfth or thirteenth the second permanent molars appear, and the last or dentes sapientiæ (wisdom teeth) seldom before eighteen or twenty, and occasionally at a much later period.
Pl. 123, fig. 18, the teeth of both jaws from before. Fig. 19, do. from the side. Fig. 20, the lower jaw of a child four years old with the milk teeth and their sockets. Fig. 21, the same for the upper jaw. Figs. 22 and 23, upper and lower jaw opened, with the milk and permanent teeth in their sockets or alveoli. Fig. 24, dental sac of a milk tooth with its vessels. Fig. 25, do. of a permanent tooth. Fig. 26, vertical section of the tooth cavity contained by the sac. Fig. 27 a–e, the teeth of the right upper jaw of a fœtus of about eight months. Fig. 28 a–e, teeth of a newborn child. [F]ig. 29 a–e, teeth of a child of four years. Fig. 30, second set of upper jaw teeth of a four years’ old child seen from within. Fig. 31, do. from below. Fig. 32, teeth of a child at seven years: A, milk teeth; B, permanent teeth. Fig. 33, teeth of a grown man. Fig. 34, the posterior molar or wisdom teeth.
4. The Palate. The palate is composed anteriorly of the palatine processes of the superior maxillary and palatine bones, covered above by the mucous membrane of the nose, and below by the lining membrane of the mouth. This portion is the hard palate, and separates the mouth from the nose. Behind it is a membranous portion called the soft palate, which partially separates the mouth from the upper part of the pharynx. The portion of the lining membrane of the mouth which covers the hard palate has a hard cartilaginous feeling, and is not so sensitive as the other parts. It has a ridge in its centre just below the middle palatine suture, and from each side there are transverse ridges extending to the alveolar processes. This arrangement is more evident anteriorly. Beneath this membrane, especially at its posterior part, the muciparous glands are very abundant and close set.
The soft palate, velum palati, is continuous with the posterior margin of the hard palate, and is stretched across the back part of the mouth from one side to the other and obliquely downwards and backwards. Its free inferior margin offers in its centre a projection about half an inch or more in length, and called the uvula. From each side of the latter there proceed two crescentic doublings of the lining membrane of the mouth called the lateral half arches of the palate. Of these the anterior is the more distinct. The tonsils are contained in the depression between these two duplicatures.
The muscles of the palate are, first, the constrictor isthmi faucium, arising from the middle of the soft palate, and inserted into the side of the tongue near its root. It tends to close the opening between the mouth and the pharynx. Second, the palato-pharyngeus, a small fasciculus within the duplicature forming the posterior lateral half arch. Extending between the soft palate and the pharynx, it serves to draw the former downwards. Third, the circumflexus or tensor palati behind the pterygoid process of the sphenoid bone. It spreads out or extends the palate. Fourth, the levator palati on the inner side of the last. It arises from the point of the petrous bone, and attached to the soft palate, draws it upwards. Fifth, the azygos uvulæ, in the centre of the soft palate and of the uvula. It arises from the ])osterior pointed termination of the middle palatine suture, and serves to draw the uvula upwards, and to diminish the vertical breadth of the soft palate.
Pl. 127, fig. 5, muscles of the palate and posterior side of the pharynx: 1, levator palati; 2, tensor palati; 3, 3′, azygos uvulæ; 4, giosso-palatine muscle; 5, constrictor isthmi; 6, posterior crico-arytenoid muscle; 7, transverse and oblique arytenoid muscles. Fig. 6, palatine muscles: 1, external pterygoid; 2, levator palati; 3, 4, tensor palati; 5, azygos uvulæ; 6, upper end of the constrictor isthmi.
5. Glands of the Mouth. The principal glands of the mouth are for the purpose of secreting saliva, a substance essential to the proper mastication, deglutition, and digestion of food. They consist of the parotid, the submaxillary, and the sublingual.
The parotid gland is the largest, and, like the rest, of a pink color. It fills up the cavity on the side of the head between the mastoid process and the ramus of the lower jaw, extending beyond the edge of the latter, so as to cover the posterior margiu of the masseter muscle. It reaches vertically downwards from the zygoma above to the angle of the jaw below. It has no appropriate capsule, but is covered by the processes from the superficial fascia of the neck. Its duct, called the duct of Steno, traverses the outer face of the masseter muscle, in a line drawn from the lobe of the ear to the tip of the nose. It is about the size of a crow-quill, and perforates the posterior part of the buccinator muscle so as to have its oral orifice opposite the second large molar tooth of the upper jaw. A small accessory gland is sometimes found between this duct and the zygoma.
The submaxillary gland is about one third the size of the parotid, and is so situated as to be bounded externally by the body of the lower jaw, superiorly by the mylo-hyoid muscle, and inferiorly by the tendon of the digastric. Its duct (ductus Whartonianus) terminates by a small projecting orifice on the anterior margin of the frsenum of the tongue.
The sublingual gland is an oblong body, visible on turning up the tongue, where it is seen as a projecting ridged substance on the under surface of the tongue. Instead of a single excretory duct, it has several, sometimes twenty. Occasionally, several of them are collected into one or two principal trunks (ductus Riviniani), which open either directly into the mouth or into the duct of Wharton. The position of the salivary glands is such that they are pressed upon during mastication, by which means their salivary secretion is expressed. All consist of a congeries of smaller glands or lobes and lobules. The arteries which supply them are branches from the external carotid. Their nerves come from the fifth pair, and from the portio dura.
The tonsils, or amygdala, situated one on each side, between the half arches of the palate, constitute a series of mucous glands of irregular figure. They are very vascular, and secrete a viscid fluid, which serves to lubricate the food in its downward passage.
Pl. 129, fig. 29, salivary glands: 1, sterno-cleido-mastoid; 2, masseter muscle; 3, parotid gland; 4, accessory parotid; 5, single glandules distributed about its duct near the end; 6, genio-glossus; 7, mylo-hyoid; 8, external, 9, internal portion of the submaxillary gland; 10, ductus Whartoni; 11, upper maxillary ganglion; 12, sublingual gland.
6. The Pharynx is a large membranous cavity, placed between the cervical vertebræ and the posterior part of the nose and mouth. By means of numerous attachments on all sides, it is prevented from collapsing, and it is drawn up and down in the movements of the tongue and larynx. It consists of three coats, an external, formed by three muscles, the constrictores pharyngis, inferior, medius, and superior; an intermediate pharyngeal aponeurosis; and the internal or lining mucous membrane. This mucous membrane is continuous with that of the mouth, nares, and Eustachian tube, and is continued inferiorly as a lining to the larynx and trachea in front and to the œsophagus behind. It is studded with numerous mucous glands.
On opening the pharynx from behind, we may observe seven apertures leading from it in different directions: in the upper or nasal portions there are the two posterior nares, and on the side of each of these there is the opening of the Eustachian tube; below the velum palati there is the isthmus faucium or posterior opening of the mouth; below and behind the tongue is the opening of the glottis; and, lastly, we have the termination of the pharynx in the œsophagus.
7. The Œsophagus is the tube in front of the spine, and behind the trachea, which conducts food from the pharynx to the stomach. When inflated, it is of cylindrical shape, about an inch in diameter, and nine or ten inches long, widening towards the stomach. Like the pharynx, it consists of three coats, an external or muscular, a middle or aponeurotic, and an internal or mucous.
8. Physiology of Mastication and Deglutition. The first step in the reduction of food taken into the mouth is its mastication, and the addition of salivary matter to the divided particles. Mastication evidently is of great importance in preparing the substances to be afterwards operated on for the action of their solvent; and it exactly corresponds with the trituration to which the chemist would submit any solid matter, that he might present it in the most advantageous form to a digestive menstruum. The complete disintegration of the alimentary matter, therefore, is of great consequence; and, if imperfectly effected, the subsequent processes are liable to derangement. This derangement we continually meet with; for there is not, perhaps, a more frequent source of dyspepsia (difficult digestion) than imperfect mastication, whether resulting from the haste with which food is swallowed, or from the want of the proper instruments. The disintegration of the food, by mechanical reduction, is manifestly aided by insalivation; it is doubtful, however, to what degree the saliva has any chemical effect upon it.
When the reduction of the food in the mouth has been sufficiently accomplished, it is carried into the œsophagus by the action of deglutition. The first stage in the process is the carrying back of the food until it has passed the anterior palatine arch; this, which is effected by the approximation of the tongue and palate, is a purely voluntary movement. In the second stage the tongue is carried still further backwards, and the larynx is drawn forwards under its root, so that the epiglottis is pressed down over the rima glottidis. The muscles of the anterior palatine arch contract after the morsel has passed it, and assist its passage backwards; these, with the tongue, cut off completely the communication between the fauces and the mouth. At the same time, the muscles of the posterior palatine arch contract in such a manner as to cause the sides of the arch to approach each other like a pair of curtains, so that the passage from the fauces into the posterior nares is nearly closed by them; to the cleft between the approximated sides the uvula is applied like a valve. A sort of inclined plane, directed obliquely downwards and backwards, is thus formed, and the morsel slides along it into the pharynx, which is brought up to receive it. Some of these acts may be performed voluntarily, but the combination of the whole is instinctive. The third stage of the process, the propulsion of the food down the œsophagus, then commences. This is accomplished in the upper part, by means of the constrictors of the pharynx; and in the lower, by the muscular coat of the œsophagus itself. When the morsels are small, and are mixed with much fluid, the undulating movements from above downwards succeed each other very rapidly; this may be well observed in horses whilst drinking; large morsels, however, are frequently some time in making their way down. Each portion of food and drink is included in the contractile walls, which are closely applied to it during the whole of its transit. The gurgling sound which is observed when drink is poured down the throat of a person in articulo mortis is due to the want of this contraction. The whole of the third stage is completely involuntary. The usual peristaltic movements of the œsophagus are reversed in vomiting; and this reversion has been observed even after the separation of the stomach from the œsophagus, as a consequence of the injection of tartarized antimony into the veins. At the point where the œsophagus enters the stomach, the cardiac orifice of the latter, there is a sort of sphincter, which is usually closed. This opens when there is a sufficient pressure on it, made by accumulated food; and afterwards closes, so as to retain the food in the stomach. The opening of the cardia is one of the first acts which take place in vomiting. When the sphincter is paralyzed by the division of the pneumogastric nerve, the food regurgitates into the œsophagus.
Organs of Assimilation

The organs concerned in digesting the food, after it has been masticated and swallowed, are the stomach and intestines, assisted by various glands.
We shall precede the detailed description of the viscera of the abdomen, by a brief reference to its regions, as established by authors. The abdomen is the largest cavity in the body; it is of an oval form; its capacity, and in some degree its figure, differ at different ages, and in different subjects; it is bounded superiorly by the diaphragm, anteriorly and laterally by the abdominal muscles, inferiorly by the true and false pelvis, and posteriorly by the lumbar vertebræ, the crura of the diaphragm, and the psoæ and the quadrati lumborum muscles. Although the expression “cavity of the abdomen” is in common use, it is not correct; for during life there is no cavity, as the diaphragm and abdominal muscles, by their alternate action, keep up such a constant and uniform pressure on the viscera, that these and the parietes are always in perfect contact. The abdomen contains the peritonœum and the organs of digestion; the kidneys, renal capsules, and ureters; also the lacteals or absorbent vessels, with their glands, and the thoracic duct, the sympathetic nerves, the aorta, vena cava, and the numerous branches of these vessels. The abdomen is generally divided by writers into nine, but by some into twelve regions; by drawing two transverse lines, one between the extremities of the cartilages of the ninth or tenth ribs, and the other between the anterior superior spinous processes of the ossa ilii, we may define three regions: the epigastric above, the umbilical in the middle, and the hypogastric below; and then, by drawing a vertical line on each side, from the extremity of the eighth or ninth rib to the centre of Poupart’s ligament, or a little external to it, we shall subdivide each of these regions into three parts: the three divisions of the epigastric region are the epigastrium, or scrobiculus cordis, in the centre, and the right and left hypochondriac regions, on either side. The epigastrium is immediately below the ensiform cartilage, and the hypochondriac regions are covered by the false ribs; the lateral portions of the umbilical division are the lumbar regions; the middle of the hypogastric region is the hypogastrium; and the lateral portions are the iliac regions. The lower part of the hypogastrium is called by some the pubic region, and the lower part of each iliac division is called inguinal region, or more properly spermatic (the term inguinal being commonly applied to the upper and anterior part of the thigh), and contains the iliac vessels, and in the male the spermatic cord, and in the female the round ligament of the uterus. These divisions are somewhat arbitrary, there being no natural or fixed boundaries to these several compartments.
1. The Stomach. The stomach is the most dilated portion of the alimentary canal, its capacity, however, being very variable. It is placed between the œsophagus and the duodenum, continuous with both, and is held in its place in the abdomen by the omentum and œsophagus. When distended, the stomach exhibits a somewhat conical figure, the base to the left side, the apex to the right, the intermediate portions being somewhat curved. It then presents two extremities, the left and the right; two orifices, the cardiac and pyloric; two surfaces, an anterior and a posterior; and two edges, the lesser or concave, and the greater or convex. The left, or splenic extremity, is very large; the right, or pyloric, is much smaller, being cylindrical and convoluted like an intestine, and is distinguished from the duodenum by the circular contraction of the pylorus, to the left of which the stomach is often found dilated towards the convex border, into a little sinus called antrum pylori. The cardiac œsophageal orifice is the highest point of the stomach, and is connected to the diaphragm by the peritonæum. The pyloric orifice is between the stomach and the duodenum. It lies to the right side of the spine, and is usually in contact with the liver and gall bladder. The anterior surface of the stomach is below the xiphoid cartilage, looking upwards and forwards. The posterior surface looks backwards and downwards, forming the front of the bag of the omentum. The lesser, or concave edge, looks backwards and upwards towards the spine. The greater, or convex edge, looks forwards and downwards towards the colon.
The stomach is composed of three proper tissues: a serous, a muscular, and a mucous. These are connected together by laminæ of cellular membrane. The serous or peritonæal coat is derived from the lamina of the lesser omentum, separating at the lesser curvature, and uniting along the convex edge to form the great omentum. It does not adhere throughout, but leaves spaces, allowing the distension of the stomach and the passage of blood-vessels. The muscular coat consists of three layers; the first, or superficial, is longitudinal, continued from the longitudinal fibres of the œsophagus, and extending towards the duodenum. The second layer consists of fibres running circularly in nearly parallel rings, beginning at the left extremity. The third set of fibres take a very irregular or oblique direction, and appear as a continuation of the circular fibres of the œsophagus. The internal or mucous coat, also called villous, from its velvety appearance, is continuous with that lining, the œsophagus, and duodenum. When fresh and healthy, it is of a rosy or pinkish color. It is always thrown into folds or wrinkles, some of which are nearly parallel to the long axis of the stomach, and thus permit the distension of this organ; other folds intersect these, so as to cause an areolated appearance. At the cardiac orifice this membrane is folded longitudinally, and somewhat festooned. Corresponding to the pylorus is a circular fold, with a small aperture in the centre, the pyloric valve, encircled by a strong band of sphincter fibres; during life, when the sphincter acts, it can effectually separate the stomach from the intestine. When the stomach and duodenum are inflated and dried, the valve will be seen to present an appearance not unlike that of the iris. On carefully cleaning the inside of the stomach from all mucus, it will exhibit numerous projecting papillæ, and between them small pits or depressions, studded with minute holes. These pits are more or less circular, and most distinct towards the pyloric orifice; they secrete the gastric juice, the mucus being probably furnished by the papillæ.
The stomach is freely supplied with blood from the cœliac axis; the coronary and epiploic arteries, with the vasa brevia, inclose it in a network of inosculation. The numerous large veins enter into the portal system. The eighth nerves expand on its surface, and form a plexus round the cardiac orifice. Numerous nerves also are derived from the solar plexus of the sympathetic.
The mucous coat of the stomach secretes the peculiar anti-putrescent and powerfully solvent liquid known as the gastric juice. By its action, aided by the temperature of the body and the motion of the stomach, food introduced through the œsophagus is, after a time, converted into a grey pulpy mass termed chyme. It is probable that the saliva (mixed with which the food comes to the stomach) performs an important part in the operation of digestion.
2. The Duodenum is the next portion of the alimentary canal. It is so named from its length (from eight to nine inches), being about equal to the breadth of twelve fingers. This is the first and shortest, but most dilatable division of the small intestine; it extends from the pylorus to the root of the mesentery, where the jejunum commences. The superior transverse portion ascends from the pylorus backwards and to the right, where it makes a sudden or acute turn, and the middle or perpendicular portion then descends in front of the right kidney as low as the third lumbar vertebra; here it makes a second turn, from which the inferior transverse portion extends obliquely across the spine. The biliary and pancreatic ducts perforate the inner side of the perpendicular division of the duodenum. These pass through its coats very obliquely, and open into the intestine, sometimes separately, sometimes together, on a small papilla opposite the inferior angle. In the duodenum, the process of digestion is completed; the chyme is mixed with the bihary and pancreatic juices, and a separation takes place between the chyle and the excrementitious matter.
3. The Jejunum and Ileum Intestines are partly concealed by the omentum. There is no exact division between these two portions, the upper two fifths being named jejunum, and placed higher in the abdomen than the remaining ileum. From the duodenum the jejunum first passes forwards and to the left side; it then descends into the middle of the abdomen, is folded upon itself over and over again, extending into various regions; finally, the terminating portion of the ileum rises out of the pelvis from left to right, and joins the cœcum at an acute angle convex upwards. This portion of the intestinal tract is well supported by the mesentery, so that while possessing sufficient freedom of motion, and the power of accommodating itself to the various displacements produced by muscular action, it is securely tied in its place.
The large intestine, from four to five feet long, is divided into cœcum, colon, and rectum. It differs from the small, not only in size but in being cellular or sacculated when distended; small processes too, appendices epiploicæ, are attached to it. Three strong longitudinal muscular bands may be observed, puckering it and causing the cellular appearance.
The cœcum, or caput coli, is a cul de sac in the right iliac fossa, which it nearly fills. It joins the colon at an obtuse angle, although there is no exact limit between them. On its external surface there are three irregular protuberances, one anteriorly and the other posteriorly. The appendix vermiformis proceeds from the left side of the lower and posterior part; this is a small tortuous cul de sac about the size of a goose quill, and may be considered as representing the more highly developed cœcum of other animals. The ileum joins the left or inner side of the cœcum at an acute angle, its mucous coat protruding into the cavity of the cœcum to form two valves. The inferior or ilio-cœcal valve is the larger; it secures the ileum against regurgitation from the cœcum; the superior or ilio-colic valve is smaller, and prevents regurgitation from the colon. These two valves are united at their commissures or extremities, and from each commissure a fold is continued round on the inner side of the cœcum; these folds are the fræna or retinacula of the valves.
4. The Colon extends from the cœcum to the rectum; it is divided into four portions. The right or ascending colon extends from the cœcum to the inferior surface of the right lobe of the liver. The transverse arch of the colon turns off at a right angle from the last, and extends tortuously from the gall bladder, transversely as far as the spleen in the left hypochondrium. The left or descending colon extends from the spleen to the iliac region behind the small intestines, and the sigmoid flexure or the fourth division completes the colon to the rectum.
5. The Rectum, or straight intestine, extends from the sigmoid flexure of the colon to the anus. It is more cylindrical and Jess sacculated than the colon; it is usually found much dilated about an inch above the anus.
The mucous coat of the small intestines, although continuous with that of the stomach, yet presents some peculiarities, the most important of which is seen iu the series of permanent folds or duplicatures named valvulæ conniventes. These commence in the vertical portion of the duodenum, and increasing exist in great quantities as far as the upper half of the ileum; thev then decrease in numbers and size, and are wholly absent in the last few feet of the ileum. They are semilunar folds or arches extending round one half or more of the tube, into which they project when this is distended, like shelves. They increase the extent of surface of intestine, and delay the food in its downward passage, affording to the absorbents a better opportunity to take up the chyle. The whole mucous surface of the small intestines is furnished with follicles and mucous glands; it also presents numerous projecting processes called villi. The follicles of Lieberkuhn are simple pouches of the membrane, very small, and scattered numerously over the whole surface. The more elaborate glands present different appearances. The glands of Brunner are chiefly in the duodenum, in the submucous tissue, and surround the intestine in a lamina of white bodies. The glands of Peyer are found chiefly along the convex, part of the intestine, sometimes single, sometimes aggregated. The function of these glands is unknown. The villi are those short cylindrical or conical processes seen so abundantly on the mucous membrane of the small intestine; when examined under a lens they are found to be covered by a fine membrane in addition to the epithelium, and to contain a minute plexus of blood-vessels through the medium of which the absorption of fluids for the canal takes place. The lacteal vessels commence in each villus by small branches, but they do not open on the surface by free orifices as was at one time supposed. At the extremity of each villus are seen small vesicles during the presence of food in the intestines, disappearing when this is empty. These in all probability are developed from nuclei by absorption of matter from the descending food, and soon burst, discharging their contents inwards towards the lacteals. Free fluids are probably taken up directly by endosmosis through the veins distributed along the intestinal tract.
The mucous membrane of the large intestine differs in having no villi and no true valvulæ conniventes. Internally are seen several crests or semi-lunar folds; these, however, are formed by all the coats, and not by the mucous membrane alone as in the small intestine.
As the food is propelled onwards through the intestines, both large and small, it becomes mingled with a vast quantity of fluid (succus intestinalis), secreted by the mucous glands and follicles. In the jejunum and ileum the chyle is absorbed by their numerous villi; the length and tortuosity of the tube, and its numerous valvules conniventes, are admirably adapted to increase the extent of this secreting and absorbing surface, and at the same time to retard the progress of the food, and to penetrate and subdivide the mass, so as to search out, as it were, and extract all the nutriment or chyle it may contain. In the large intestine the contents acquire their feculent properties, the first traces of which they exhibit in the cœcum. In their passage along this part of the canal, the absorbents may probably continue to take up any chyle that may have escaped those in the ileum, as also the watery parts of the food, and the faeces become hardened by degrees, and moulded or figured according to the length of time they are lodged in the cells of the colon. The great length of this tube, as well as its yielding structure, adapt it as a reservoir capable of retaining a considerable quantity, and thus obviating the inconvenience of frequent defecation. The rectum also contributes to the same effect, being retained in a closed state by the sphincters and supported by the levatores ani muscles. When the evacuation of the bowels is called for by the peculiar sensations in the part, the contents are expelled partly by the muscular action of the rectum and the concurring relaxation of its sphincter, aided by the voluntary contraction of the diaphragm and abdominal muscles.
Pl. 130, fig. 11, stomach with its fleshy fibres: 1, 2, longitudinal fibres from the cardiac orifice; 3, circular and transverse fibres. Fig. 12, œsophagus at its entrance into the stomach: 1, mucous membrane of the œsophagus; 2, do. of the stomach; 3, line of separation between the two; the inequalities indicate the cardiac orifice. Fig. 13, valve of the pylorus. Fig. 14, intestinal tract: 1, coils of the small intestines; 2, cœcum with its vermicular appendage; 3, ascending, 4, transverse, 5, descending colon; 6, sigmoid flexure; 7, rectum; 8, appendices epiploicæ, folds of the peritonæum filled with fat. Fig. 15, portion of the small intestines opened to show the valvulæ conniventes. Fig. 16, cœcum opened: 1, end of the ileum; 2, vermicular appendage; 3, its opening into the cœcum; 4, opening of the ileum; 5, 6, folds of the mucous membranes, forming the lips of the valves.
The glandular viscera of the abdomen which are subservient to digestion and assimilation are, the liver, spleen, and pancreas.
6. The Liver is the Ingest and heaviest secreting gland in the body; it is situated below the diaphragm, and above the right kidney, the stomach, duodenum, and lesser omentum; and is supported in this position by several folds of the peritonœum, inaccurately termed ligaments, viz. the falciform, round, right, left, and coronary. These connect it to the diaphragm and to the abdominal muscles, and the lesser omentum attaches it to the stomach and omentum. Its weight varies from three to five pounds, depending on the amount of blood included; its transverse diameter is about ten or twelve inches, the vertical about seven in the deepest part of the right lobe.
The liver is of very irregular form. The superior or anterior surface is smooth, and convex, and divided by the suspensory ligament into a right and left portion. The inferior surface looks backwards and downwards; it is very irregular, and marked by several projections and depressions. The former are called lobes, and are five in number: first, the great or right lobe; secondly, the left lobe, which rests on the stomach; third, the spigelian or middle lobe, situated behind the lesser omentum; fourth, the lobulus caudatus, immediately behind the transverse fissure; fifth, the lobulus quadratus or anonymus, at the anterior part of the right lobe.
The principal depressions or fissures on the inferior surface of the liver are: the transverse fissure or porta, situated between the lobulus quadratus and caudatus; the horizontal fissure, extending from the notch in the anterior edge of the liver upwards between the right and left lobes; the fissure for the vena cava, between the lobulus spigelii and the right lobe; the depression of the gall bladder, to the right of the lobulus quadratus; two superficial depressions on the under side of the right lobe; a superficial depression on the under surface of the left lobe; and lastly, a broad notch in the posterior edge of the liver. Several notches may be observed in the circumference of the liver.
The liver is of a peculiar brown color, mottled with yellow, and consists of numerous small granulations or lobules, connected together by branches of the hepatic arteries and veins, and of the vena porta and biliary ducts, and by lymphatics and nerves, the whole cemented together by a fibrous coat which covers the surface, and sends inwards numerous subdividing laminæ so as to form a capsule for each lobule. This coat also accompanies the three vessels of the liver which enter or leave the transverse fissure, and forms a sheath round their ramifications throughout the entire organ, known as Glisson’s capsule. The lobules are small granules, composed of a plexus of biliary ducts, of a portal venous plexus, of an interlobular branch of an hepatic vein, and of minute arteries. The circulation of blood in the liver has already been described under the vascular system. The venous blood from the vena porta is brought to this organ and distributed throughout its substance. There it is subjected to certain influences which result in the elaboration of bile, which, after collecting from innumerable fine canals, flows into the hepatic ducts which unite into a common hepatic duct. This duct descends for about an inch and a half along the lesser omentum, and is then joined at an acute angle by the cystic duct from the gall bladder; the union of the two forms the ductus choledochus communis. The latter duct, about three and a half inches long, perforates the coats of the duodenum very obliquely opposite to its lower angle; here it is usually joined on the left side by the duct from the pancreas.
The gall bladder is a pear-shaped reservoir, the neck of which is extended into the cystic duct, which joins the hepatic duct at an acute angle to form the choledochus communis. It serves to retain the bile when not wanted in the intestinal canal; when pressed upon by the presence of food in the duodenum, its contents are forced out through the cystic duct and the ductus communis. Bile may pass directly from the liver to the intestines without entering the gall bladder at all.
7. The Spleen is a soft spongy mass, situated between the stomach and ribs, beneath the diaphragm, and above the kidney and colon. It has no excretory duct, but its vein joins the vena porta directly, and it may therefore be considered as accessory to the liver in its function of depuration. Its precise office, however, is not known. On the concave surface, turned towards the stomach, there is a central depression or fissure, termed the hilum.
8. The Pancreas, or sweetbread, lies behind the stomach. It is a conglomerate gland, very similar in appearance and texture to the salivary glands. It is flat, thin, and elongated, about seven inches long and an inch and a half broad. The middle portion is called the body; the splenic or left extremity is the tail; the right, broad and flat, is the head. The pancreatic duct commences at the small end, and extends to the large, receiving numerous branches on each side. It generally joins the ductus choledochus in a small dilatation just before the duodenal opening; a second duct sometimes opens directly into the duodenum. An accessory gland, called the lesser pancreas, is sometimes found attached to the head of the pancreas. The pancreatic juice is mixed with the biliary in the duodenum, to separate chyle from the chyme of the food. Its especial office, from recent investigations, appears to lie in the assimilation of fats.
9. The Peritonæum. The peritonœum is the largest serous membrane in the body, investing the viscera of the abdomen, much as those of the thorax are embraced by the pleura. The peritona3um is a closed sac, and when opened, presents a continuous surface, which may be traced throughout the whole extent without interruption. The different folds which the peritonæum forms in its course are mainly the lesser omentum, the great omentum, the splenic omentum, the colic omentum, the appendices epiploicæ, the mesentery, meso-cœcum, and meso-rectum. The relations of the peritonseum in the different parts of its course will be best understood by reference to pl. 130, fig. 9.
Proceeding from the umbilicus, 1, the peritonasum passes along the inside of the anterior abdominal wall, 2; then bending backwards, it lines the inferior surface of the diaphragm, 3, forming on it the suspensory ligament, 4, of the liver, 5; it passes below the diaphragm over the liver, and coats its upper surface, 6, the gall bladder, 7, and a portion of the lower surface of the liver. From the liver it passes to the stomach, and forms, 8, the anterior lamina of the lesser or gastro-hepatic omentum, and passes from the stomach to the spleen as the anterior lamina of the gastro-splenic ligament. The peritonæum next bends back on itself from the diaphragm in the form of a sac (saccus cpiploicus), the opening, 10, to which is known as the foramen of Winslow. The two laminæ of the gastro-hepatic omentum separate at the lesser arch of the stomach, 11, to inclose this organ, the posterior layer giving a serous covering to its back part, and the anterior to its fore part; they then touch each other again, 12, along the great arch of the stomach, and being joined by the peritonœum from the spleen and the splenic vessels, descend to the lower part of the abdomen under the name of the gastro-colic or the great omentum, 13. This then turns on itself and ascends obliquely backwards to the arch of the colon, along the convex edge of which its laminæ separate to inclose this intestine, 14, and its vessels. Along the concave edge of the colon these laminæ again unite, 15, to form the transverse meso-colon which passes backwards to the spine. Opposite the duodenum, 16, this process separates into an ascending and descending layer, between which the inferior division of the duodenum lies. The ascending layer covers the pancreas, 17, and proceeding to the back part of the right lobe of the liver, becomes continuous with the peritonæal layer, 18, of this viscus. The descending layer, 19, of the transverse meso-colon expands in each lumbar region, in which it attaches the lumbar portion of the colon by a duplicature called the right and left lumbar meso-colon; it is thence reflected forwards over the small intestines, 20, 20, and returns again to the spine, forming the remarkable plaited process, the mesentery, 21, 21, Inferiorly it covers the sigmoid flexure, 22, and a portion of the rectum, 23, forms duplicate folds, 24, between the rectum and uterus, covers the uterus itself, 25, and constitutes on each side the broad ligament, 26, 26, subdivided anteriorly into three smaller folds, containing the round ligament, the Fallopian tube, and the ovary. It next passes to the posterior surface of the bladder, 27, forms here a few folds, 28, returns to the umbilicus, covers the umbilical vessels, 29, and contributes, 30, to the formation of the lateral ligaments of the bladder. Fig. 10, anterior view of the stomach, duodenum, and omentum majus; the posterior portion of the reflected liver is shown: 1, stomach; 2, lower border of the stomach; 3, pyloric extremity; 4, cardiac do.; 5, pylorus; 6, duodenum; 7, head of the pancreas; 8, 9, portion of the large intestines; 10, portion of the omentum majus; 11, lower surface of the right lobe of the liver; 12, inferior vena cava; 13, left longitudinal fissure, with the obliterated umbilical vein; 14, transverse furrow or porta, with the vessels; 15, gall bladder and cystic duct, uniting with the hepatic duct into the ductus choledochus communis; 17, trunk of the portal vein; 18, hepatic artery; 19, lobulus quadratus; 20, spigehan lobe; 21, left lobe of the liver. Fig. 17, spleen: 1, 2, furrow on the convex side; 3, 4, opening for vessels in the concave side. Fig. 18, biliary duct, gall bladder, and pancreas: 1, duodenum; 2, gall bladder opened; 3, the small spiral folds of the neck; 4, cystic duct; 5, hepatic duct; 6, common duct; 7, pancreas; 8, right extremity; 9, pancreatic duct.
![]() Urinary Organs
Urinary Organs
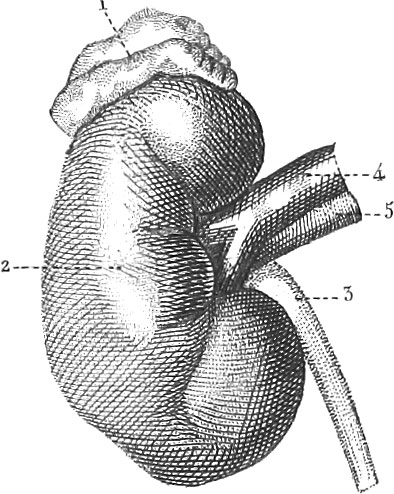 Urinary Organs
Urinary OrgansAs many substances are introduced into the system which are either unnecessary or injurious, some means must be devised to remove them from the blood, into which they have been carried, as well as to separate effete particles from the system itself. The skin and the lungs perform much of this office, but the greater share is to be attributed to the urinary apparatus. This consists of the two kidneys which secrete the urine; the two excretory ducts, the ureters, which convey the urine to the uriuary bladder, a temporary reservoir; finally, the urethra, which discharges it externally, and which in the male is common to both the urinary and the genital organs.
1. The Kidneys present the well known shape of the kidney bean, and are about four inches in length, two in breadth, and one in thickness. The external surface is smooth, and invested by a capsule, which is attached so loosely as to permit of being readily peeled off. A deep notch on the concave edge of the kidney serves for the passage of its vessels, and marks the hilum. The superior end of each kidney is surmounted by the suprarenal body.
A vertical section of a kidney from the convex edge to the concave, will show it to consist of two entirely different substances, an external or vascular and an internal or membranous. The external vascular or cortical substance forms the superficial lanuna of the gland, is about two lines thick, and sends long prolongations inwards between the membranous fasciculi. A microscopical examination shows the cortex to be composed of numerous arterial and venous ramifications, entangled with convoluted uriniferous tubes (tubes of Ferrein); an immense number of small granules may also be detected. These are the corpora or acini of Malpighi. A Malpighian corpus or corpuscle is a tuft of capillary arteries, arranged in loops, close pressed together, and inclosed in a slight dilatation of the urinary tube, which thus forms a capsule to it. A small artery called vas inferens pierces this capsule, and then divides into the branches which are coiled up to form this minute vascular ball, from the interior of which a small vein (vas efferens) proceeds, smaller than the artery, and piercing the capsule close to it, enters the venous plexus surrounding the convoluted uriniferous tubes, and from which the blood is ultimately conveyed out of the kidneys by the renal or emulgent vein. We have thus two distinct systems of capillary vessels, tli rough both of which the blood passes in its course from the arteries to the veins. The first is an arterial capillary system, forming the Malpighian tufts, contained within the uriniferous tubes; the second is the venous plexus which surrounds these convoluted tubes. It has been supposed that the former serve to liberate water and the more simple elements of the blood, while the latter eliminate the more complex urea, uric acid, &c.
The tubular substance is internal to the cortex, and consists of fine vessels arranged in about fifteen pyramids; the bases directed outwards, the apices towards the hilum. At and near the apex these vessels are straight, but, proceeding outwards, they communicate; and, on entering the cortical substance, become twisted and convoluted in the most complicated manner.
The papillæ, or the mammillary processes, form the apices of the cones. Each is perforated by a number of fine holes, the orifices of the individual tubes, and through which the urine flows when these are compressed. The extremities of the papillæ are embraced by the calyces, membranous cups which unite with each other at the other end to form the ureter. Those calyces of each extremity, as well as those in the centre, unite into the three small tubes, the infundibida, which, after a short course, terminate in the pelvis an oval flattened reservoir, which is continued into the ureter.
2. The Ureter is the excretory duct of the kidney, and extends to the urinary bladder. Each ureter is about eighteen inches long, and of the thickness of a goose-quill. They enter the bladder by passing obliquely between its muscular and mucous coats.
Attached to the upper extremity of each kidney is a small gland-like body, termed renal capsule, or supra-renal body. They are well supplied with vessels, but do not appear to be especially connected with the kidneys. Their use is unknown, although it is probable that with the thymus and thyroid bodies they are concerned most especially in the economy of the fœtus.
3. The Bladder, vesica urinaria, is the reservoir of the urine, which constantly trickles into it from the ureters. It lies behind the pubes, and rests on the rectum. It possesses muscular fibres, and a cervical sphincter. The different regions have received different names, as the superior fundus, for the superior anterior extremity; inferior fundus, the posterior extremity resting on the rectum; the body, the intervening portion; and the cervix, the portion connected with the pubes, above the rectum.
4. The Urethra. The urine is discharged from the bladder by the urethra, a membranous tube, which in the male extends to the extremity of the penis; and in the female opens into the vagina, behind and below the clitoris.
The principal constituent of urine is water. When evaporated, the residuum consists principally of urea, uric and hippuric acids; substances containing a very large amount of nitrogen. Food, mode of life, &c., greatly affect the nature of the urine. The presence of lactic acid is denied by some authors. Extractive matters are present, especially during a vegetable diet, also certain mineral substances, as phosphoric and sulphuric acids, alkaline carbonates, earthy phosphates, and chlorides; The sulphuric acid combinations enter in greatest amount, and to a larger extent, under a purely animal diet, than when the food is more miscellaneous.
Urine is generally acid; occasionally, however, it is alkaline, and it always exhibits a conversion of its urea into carbonate of ammonia during putrefaction. Certain substances are readily eliminated from the blood by the kidneys; others with more difficulty or not at all. Alcohol, sulphuric ether, camphor, musk, and many vegetable colors, are not removed from the blood. On the other hand, carbonates, sulphates, chlorates, and nitrates of potassa, coloring matter of indigo, musk, castoreum, assafœtida, &c., are entirely separated. An intermediate class undergoes a transformation before elimination.
Pl. 130, fig. 19, exterior of a kidney: 1, supra-renal body; 2, kidney; 3, ureter; 4, 5, artery and vein. Fig. 20, section of a kidney: 1, cortical substance; 2, a Malpighian pyramid, composed of uriniferous tubercles and the pyramids of Ferrein, with the papillæ; 3, a calyx; 4, pelvis; 5, ureter. Fig. 21, bladder: 1, muscular layer, with its differently arranged fibres; 1′,neck of the bladder, with its sphincter muscle; 2, 3, ureters; 4, suspensory ligament from the peritonasum; 5, vesicula seminalis; 6, prostate gland; 7, portion of the urethra.
![]() Surgery
Surgery
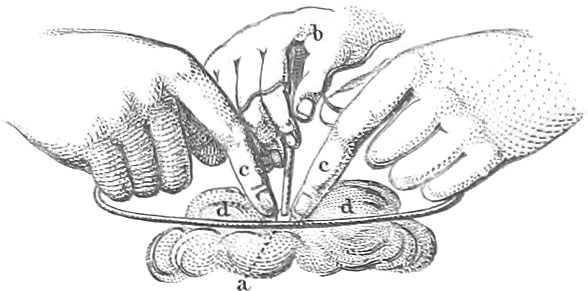 Surgery
SurgeryBy Surgery is to be understood that portion of the Healing Art which seeks to remedy such diseases and malformations of the human body as can be affected by external applications, whether they be medicines or instruments, &c.; keeping, however, in mind that internal medicines acting upon the whole system, and a proper diet, are almost always to be conjoined.
The following preliminaries to every surgical operation are carefully to be borne in mind: The system of the patient, as well as his mind, must first receive proper preparation. When possible, sufficient and skilful assistance must be at hand; the location and the position of the patient must be suitable both for the individual and the operator; all necessary apparatus, instruments, bandages, &c., must be in proper order and prepared for all emergencies; finally, the operation must be finished as quickly as possible, to relieve the patient from pain.
As it is the pain of a surgical operation that is most dreaded by the patient, due attention should be directed to alleviating this as much as possible. To this end various means may be employed; such as compression of the nerves between the part to be operated upon and the brain, which may be effected partly by the hands, and partly by means of instruments. Narcotic appliances, as opium, are also used for the same purpose. In the use of sharp instruments, they should be perfectly sharp and free from rust, and. every instrument, before being used, should be heated slightly and rubbed with fresh olive oil: the application of this substance not only diminishes pain, and increases the sharpness of cutting instruments, but also facilitates the introduction of such as are blunt. Quite recently the inhalation of ether and chloroform has been used as an anaesthetic agency to the greatest advantage. To give a complete description of all surgical instruments now in use would require many volumes, as every operator has forms peculiar to himself We shall restrict ourselves to a brief notice of such as are most generally employed, considering them under the heads of the principal varieties of operations. Instruments almost always in the hands of the operator are lancets, trochars, knives of the most varied forms, hooks, probes, sondes, forceps, nippers, scissors, saws, chisels, hammers, needles, &c. Figures of some of these are given on pl. 140. Fig. 1, usual form of thumb lancet; fig. 2, Spanish lancet; fig. 3, abscess lancet; fig. 4, Petit’s trochar, with the canula; fig. 11, common tenaculum; fig. 13, simple button-headed sound; fig. 14, common forceps; fig. 16, straight scissors; fig. 17, curved scissors.


Blood-Letting
Blood-letting is made use of partly to diminish the amount in the system, and partly to restore circulation and to conduct it to or from some particular region. It thus comes into play in such, diseases as plethora, inflammation, congestion, cramps, fever, &c. The principal methods of extracting blood are as follows.
1. Scarification. This consists in making numerous superficial incisions in the skin of a particular spot with a lancet (pl. 140, figs. 1 and 2), or with some special apparatus, for the purpose of removing fluids from the capillaries or from the cellular tissue.
A convenient instrument for this purpose is known as the scarificator (fig. 31 a b), which consists of a cubical brass box in which ten to sixteen lancets turn on a common pivot so as to have their points project above the surface; the extent of their projection is regulated by a screw. On drawing back the handle, the lancets disappear beneath the surface and are there held by a spring. Bringing the scarificator over a given spot, and loosening the spring, the lancets will all fly out at once, and produce as many delicate incisions. The operation of cupping is usually connected with the use of this instrument, and is intended to facilitate the flow of the fluids to be extracted. The cups, consisting of little bells of glass, are laid over the spot scarified, and the included air exhausted by means of a burning piece of paper, previously introduced. The pressure of the external air causes the blood to flow freely. Sometimes the exhaustion is produced by means of a small air-pump.
2. Venesection, or Blood-Letting, is a time-honored operation, constantly brought into requisition; it consists in opening a single vein, and permitting as much blood to flow therefrom as may be desirable.
The surgical apparatus necessary in blood-letting includes a soft linen bandage of about a yard in length and two inches in breadth; a bleeding lancet (fig. 1), which, in the hands of a skilful operator, has great advantages over the spring lancet; a compress formed of a roll of linen about a yard long and two inches broad; proper vessels for receiving the blood; a soft sponge, and clean lukewarm water.
Bleeding with the spring lancet (fig. 32 a b), the common spring lancet; fig. 33, the lancet of Walbaum; fig. 34, the lancet of Perret, a, b, c, various blades) requires the same preparations as with the common lancet. After the vein has been prepared, the spring of the lancet is to be set, and the blade brought over the spot where the incision is to be made. On touching the spring, the blade is liberated and pierces the vein.
Pl. 139, fig. 1, bend of the elbow or the usual spot for blood-letting, the skin supposed to be removed: 1, trunk of the basilic vein in the depression along the inner border of the biceps brachii; 2, cephalic vein on the outer side of the biceps, and separated from the nerve by the fascia; 3, 3, basilic and cephalic veins on the forearm; 4, a probe introduced under the brachial artery; 5, median vein which communicates with the deep vein in front of the opening in the aponeurotic membrane, and divides above to unite by a short branch (median cephalic) with the cephalic vein, and by a longer branch (median basilic) with the basilic vein; 6, superficial posterior basilic vein; 7, superficial posterior cephalic vein; 8, trunk of the great internal brachial nerve on the inside of the basilic vein; 9, muscular cutaneous nerve dividing principally about the median vein; 10, aponeurotic strip, which, proceeding from the tendon of the biceps, overlies the brachial artery and vein, and median nerve, and passes into the radial side of the fascia of the forearm; 12, 12, 12, circumference of the opening in the aponeurosis, well defined internally, but externally confounded with the cellular tissue; 13, 13, brachial artery; 14, radial artery; 15, ulnar artery; 16, median nerve; 17, 17, brachial vein; 18 and 20, 20, outer muscles, and 19, 19, inner muscles of the forearm; 21, internal condyle of the elbow; 22, a hook by which the opening in the fascia is drawn inwards to show, above the tendinous strip of the biceps, the brachial artery and vein, the median nerve, the brachiseus intern us muscle, and the protractor teres; 23, everted skin with adipose tissue; 24, skin of the forearm; 25, skin of the arm.
In inflammation of deep-seated parts, especially such as threaten suppuration, and even when this has already commenced, powerful counter-irritants are frequently necessary and advisable; these may consist in the introduction of setons, in the use of caustics, or the still more severe application of the actual cautery with red hot iron, and of moxas. The irons used in cauterization differ much in form. We shall here only mention the prismatic cautery of Larrey (pl. 140, fig. 38), whose prism has a narrow base in proportion to its height, and has the anterior corners cut off obliquely; also the prismatic cautery of Rust (fig. 39), which is 1 inch 4 lines long and has three equal surfaces \(\frac{3}{4}\) of an inch in breadth.
3. Acupuncture is an operation which has for a long time been successfully used in various ailments, as rheumatism, gout, &c. It consists in repeatedly piercing the part affected with a long needle, moving it backwards and forwards in the wound.
Sarlaridere’s galvanic acupuncture needle (figs. 40, 41).
Sewing up of Wounds, or Sutura Cuenta
Wounds are of various sorts: they are punctured, when produced by a pointed instrument; incised, when made by a cutting instrument; lacerated, when the parts are lacerated or torn; poisoned, when some virulent substance has been introduced; contused, when made by a blunt body, as a bullet. Incised and punctured wounds are of most frequent occurrence, and formerly were almost entirely treated by sewing up the edges; more inodern surgery, however, rarely uses anything else than sticking-plaster and proper bandages, by which the lips of the wound are more closely approximated and the reparative powers of the system less interfered with. The following sutures are those most employed at the present day, when at all necessary.
1. The Interrupted Suture, sutura nodosa (pl. 140, fig. 28). This requires as many ligature needles as there are ligatures, the needles being of various shapes to suit the emergency (fig. 25, the ligature needle of Assolini; fig. 26, do. of Blasius; fig. 27, do. of Savigny). Each needle is to be provided with one or more turns of thread, as the case may require. After the wound has been cleaned and the flow of blood has ceased, the point of the needle is to be passed through the lips of the wound previously brought into contact, and the two ends of the thread tied in a simple or a slip knot; the knot, however, should not rest directly on the edge of the wound. Each end of the thread or ligature may be provided with a needle, and the needles be introduced to the bottom of the wound and passed outwards on each side. After tying the knot, the ends of the thread may be fastened down to the skin with plaster; a similar strip should be laid between the ligatures, a roll of lint coated with cerate placed on the wound, upon this a compress, and finally a suitable bandage.
2. The Twisted Hair Pin, or Figure-of-Eight Suture (fig. 29), is the suture usually employed in cases of hare-lip. Straight hair-pin needles are introduced at suitable distances through both edges of the wound, and after the lips have been brought into contact, a thread is wound round the pin from one side to the other, in a figure-of-eight manner.
3. The Quill Suture (fig. 30) is an interrupted suture with the threads tied over rolls of adhesive plaster, or quills, which thus supply the place of the lateral compresses.
It frequently becomes necessary to employ instruments in the opening of abscesses, or collections of pus, which may exist in different parts of the body. The incision is usually made on the most protruding portion by means of a lancet (figs. 1–3), or a scalpel (figs. 7, 8); a sharp bistoury (fig. 9) may also be employed. Should the abscess be deep, a trochar may be required (fig. 4, Petit’s trochar and canula). This consists of a steel rod or stylet fitting accurately into the hollow cylinder or canula, beyond whose extremity its point projects. The puncture is made with the stylet in the canula, and on removing the former, the fluid passes out through the latter.
Sometimes the pus from an abscess escapes between the soft parts of the body by a longer or shorter channel, which ultimately opens outwards, producing a fistula. These fistulous canals require to be opened throughout their entire length by a bistoury (pl. 140, fig. 9, sharp bistoury; fig. 10, blunt bistoury).
Aneurism
By aneurism is meant a dilatation of an artery in some particular spot, producing a tumor, which will be likely to burst in time, unless the proper precautions are made use of. These precautions consist essentially in obstructing the flow of blood through the artery at the spot affected.
Among the instruments necessary in operations for aneurism may be mentioned the tourniquet: figs. 86, 87, Henkel’s field tourniquet; fig. 88, Savigny’s tourniquet; various knives, sounds, needles, compresses, ligatures of waxed silk, tenacula, forceps (as fig. 15), scissors, &c., together with the necessary bandages.
The apparatus necessary for tying an artery is much like that required in operations for aneurism: a straight edged scalpel (fig. 5), a Bromfield tenaculum artery forceps, aneurismal needle, &c. The artery is to be elevated by a tenaculum or forceps at or near the spot where the ligature is to be applied, and this passed beneath or over the artery to be severed and tied by an assistant (pl. 139, fig. 3, a, the vessel held by the surgeon with the forceps, b, the thread, d, d, passed round, and the knot tied by the assistant).
Sometimes a vessel is tied by simply passing a thread round it, without laying it bare, the extremities of the thread being then tied tightly together. Pl. 139, fig. 2, a, the bleeding vessel; b, c, points where the needle is first passed in and out; d, e, points where this is done a second time.
The method of torsion consists in twisting the extremity of the severed vessel several times round with sliding forceps (pl. 140, figs. 35, 36, 37).
Pl. 139, fig. 4, is intended to show the usual points of incision either in tying wounded arteries, or in performing operations on aneurism: a b, incision for laying bare the superior thyroid artery, which begins near the angle of the lower jaw, over the submaxillary gland, and descends an inch and a half to the lower border of the thyroid cartilage; c d, incision for exposing the carotid artery. This, two and a half inches long, passes along the inner border of the sterno-cleido-mastoid; e f, Zang’s incision for the same purpose as the last. It descends from the top of the cricoid cartilage, between the two portions of the sterno-cleido-mastoid on its outer margin, and ends one quarter of an inch above the clavicle; g h, Zang’s incision for exposing the subclavian artery above the clavicle. It commences two inches above the clavicle, on the posterior margin of the sternal extremity of the sterno-cleido-mastoid, and passes obliquely downwards and outwards to the middle of the upper margin of the clavicle; i k, Hodgson’s incision for the same purpose as the last, along the upper margin of the clavicle, to the point of attachment of the trapezius to the clavicle; l m, incision for exposing the subclavian along the inner margin of the scalenus anticus immediately over the sternal end of the clavicle, three inches long; n o, incision for exposing the subclavian beneath the clavicle; q r, Rust and Zang’s incision for the same purpose; s t, Lisfranc’s incision for exposing the axillary artery in the axilla; u v, incision for the brachial artery in the middle of the arm; w x, incision in the left arm for the same purpose, a little higher up; y z, incision for the same purpose in the bend of the elbow; 1, 2, incision for the radial artery along the upper portion of the forearm; 3, 4, the radial artery over the carpus; 5, 6, the ulnar artery in the superior portion of the forearm; 7, 8, ulnar artery over the carpus; 9, 10, incision for the descending artery according to Cooper; 11, 12, internal iliac after Stevens; 13, 14, do. after Abernethy and Scarpa; 15, 16, do. after Cooper; 17, 18, for exposing the crural artery below the groin; 19, 20, do. in the middle of the thigh; 21, 22, the posterior tibial artery along the upper third of the leg after Marjolin; 23, 24, do. in the middle of the leg, after Lisfranc; 29, 30, do. behind the inner ankle; 25, 26, incision for the anterior tibial in the middle of the leg; 27, 28, do. in the lower part of the leg.
Tying of the common carotid, after Zang, pl. 139, fig. 5; a, b, incision laying bare the carotid artery: 1, sternal, 2, clavicular portions of the sterno-cleido-mastoid muscle; 3, omo-hyoid muscle; 4, rectus capitis anticus major muscle; 5, portion of the thyroid gland; 6, sheath surrounding the carotid artery and internal jugular vein, a portion of it removed; 7, common carotid; 8, internal jugular.
Tying of the axillary artery in the left axilla, fig. 6 a; a, b, incision exposing the artery: a, axillary artery; b, external thoracic artery; h, external thoracic vein; o, musciilo-cutaneous nerve; p, median nerve; q, ulnar nerve. In the region of the incision, b b, external thoracic artery; c, subscapularis artery; d, posterior circumflex scapular artery; e, anterior do.; h, external thoracic vein; i, subclavian vein; k, posterior, l, anterior circumflex scapular vein; m, brachial vein; n, ulnar vein; r, median cutaneous nerve of the arm.
Tying of the brachial artery in the middle of the arm, fig. 6 b, a, b, incision: 1, musculo-cutaneous nerve; 2, median nerve; 3, brachial artery; 4, radial nerve: 5, brachial vein.
Trepanning
The penetration of the cavity of the cranium by sawing out a circular poition of its walls (trepanatio cranii) belongs to the earliest surgical operations.
The principal instrument required is the one known as the trepan or trephine, of which innumerable modifications have at different times been constructed. The curved or brace trepan is shown in pl. 140, fig. 62. This consists of a handle part and two extremities. The handle, a, is a cylindrical steel rod, about four inches long, and surrounded by ebony three quarters of an inch thick in the middle, tapering towards the ends, and attached nearly at a right angle to the two arms. The upper arm, b, is of steel, three and a quarter inches long, and consisting of two equal arcs; at its anterior extremity is the perpendicular steel portion, c, one inch long and five lines thick, thickened and blunt below, and turned off above so as to present a cylindrical pin an inch and a half long, ending with a short four-sided female screw, and when in use connected with the head, k. The cylindrical portion, f, of the head is twenty lines long, strongest superiorly, with a screw collar above of three lines in length, and pierced by a cylindrical canal which fits over the pin, d. The superior portion of the canal receives the disk, g, which, with its quadrangular hole, is placed over the female screw of the pin, d, and fastened by the screw, h, in such a manner that the cylinder cannot come off from the pin. The button, i, is a circular disk, two inches broad, rounded off on both sides, having in its inferior surface a screw cavity which fits over the male screw out on the upper end of f. The lower arm, l, is like the upper, and at its anterior extremity is provided with a cylindrical tube, m, seventeen lines long, and six broad. This, at its lower end, has a four-cornered cavity, n, for the reception of the shaft of the perforator, which is held in place by the small spring, o, worked by an external lever, p,
Bichat’s trepan, fig. 63, consists of a handle part, b, surmounted by a head, a, and to whose lower end, instead of a tube, is attached a hexagonal rod, which by means of an offset enters the four-sided pointed pyramid, c. In the roof of the crown is fastened an octagonal elongated nut, perforated longitudinally (with the roof) by a four-sided canal, corresponding to the pyramid, c. The pyramid is slipped into the nut of the crown, and this held at any position on the pyramid by means of a screw passing through the side of the nut. The crown is cylindrical, with vertical angular grooves, corresponding to the teeth cut on its cylindrical extremity.
The hand trepan, or trephine (fig. 64, crown 63 bc) consists of a perforator with movable central axis, handle, and screw. The handle, a, a, is of ebony, three and a half inches long. It is perforated in the centre for the reception of the shaft of the perforator. This shaft is hollow, and in it plays a pointed centre pin, the extremity of which corresponds to the centre of the circle of serrations, and which may be fixed at any point by a screw in the shaft.
The crowns of the perforator vary in shape. The old conical crown (fig. 65) is much like the next mentioned, and also provided with a centre pin, but more conical and with fewer sharp ridges on the side. The conical ridged crown (fig. 66) has the ridges equal in number and corresponding to the teeth, but diverging from each other superiorly. The cylindrical ridged crown (fig. 67) has teeth forming right angled triangles, so arranged as only to cut when turned in one direction.
A peculiarly constructed instrument called Kittel’s crank trepan and circular saw is shown in fig. 68. The general features of the instrument will be readily understood from a simple inspection of the figure, c represents an arrangement by which the circular saw t can be employed. s is the central pin or pyramid of the perforator. b, a key for screwing this in or out.
After the hair has been removed from the wounded part of the cranium, three assistants stationed near, and the position of the patient settled, the bone is next to be laid bare. This is done by making a T or Y shaped or oval incision, and reflecting the flaps.
The perforation of the cranium comes next in order. The brace trepan has here the advantage of the trephine. The centre pin or point of the pyramid is made to project slightly beyond the cutting plane of the crown, and is fixed by the screw. The operation is now to be commenced, and continued only until the teeth of the crown have made a well defined groove, when the centre pin is to be withdrawn or pushed up. The operation is then continued cautiously, care being taken to examine the groove frequently with a probe to ascertain whether it has reached the dura mater. To prevent splintering of the inner table of the cranium, the groove after penetrating the cranium may be smoothed off with a knife having a knob or button at the point (as shown in fig. 10).
Operations on the Eye
Few parts of the body are exposed to such manifold evils as the eye. Great progress has been made by modern surgery in the treatment of this organ, and if in some cases its aid be ineffectual, in others every desirable result has been accomplished.
1. Affections of the Lachrymal Apparatus. A defective condition of the punctsf lachrymalia and lachrymal canals and nasal duct is shown by a constant overflow of tears. Various operations have been made use of to restore the flow of the lachrymal secretion through these natural channels. Anel invented a syringe (pl. 140, fig. 50) the fine point of which is introduced into the puncta, and an injection of lukewarm water forced through. This syringe (from \(\frac{1}{4}\) to 1 oz. capacity) is made either of silver or of glass; the exceedingly fine tubes, of gold, silver, or steel. Fig. 54 represents a peculiar jet piece as used by Laforest.
Operations frequently become necessary for obstruction of the nasal duct, caused by accumulation of matter, contraction of the parietes, or even by the entire absence of the bony canal. In fistula lachrymalis it becomes necessary to open the lachrymal sac for the purpose of restoring the function of the duct. For this purpose is used a small scalpel (Rutdorfer’s fistula scalpel), the point of which is introduced deep enough into the part affected to overcome any slight resistance (pl. 139, fig. 8 a); the incision is then to be widened, and the fistula opened, if present. A blunt probe is next to be pushed into the nasal duct (fig. 8 b, and pl. 140, fig. 53); should this meet with any obstruction, so as absolutely to bar its passage, a sharp probe is to be employed to pierce through this obstruction, and so to open the duct.
The restoration of the nasal duct is much preferable to the formation of an artificial one; cases do occur, however, where the latter is alone possible. After the lachrymal sac is opened, a trochar (fig. 56, Bell’s trochar) is introduced through the lachrymal bone, and turned round until it penetrates the nasal cavity. After inflammation has subsided, a style of silver or a piece of catgut bougie may be introduced into the aperture.
Pl. 139, fig. 7, after Scarpa, illustrates the position of the lachrymal sac.
Among diseases of the eyelids requiring an operation, we find entropion or permanent inversion of the eyelids, and with it the turning in of the eyelashes. By means of an anatomical forceps, or an entropial forceps (pl. 140, fig. 48), a fold of the skin of the eyelids is taken up sufficiently large to bring the edge of the lid and the cilia in their normal position; this fold is then to be cut off with a pair of scissors, paid the edges brought together, The inversion will usually be counteracted by the resulting cicatrix.
It sometimes becomes necessary to cut off the whole eyelid with the roots of the cilia. A thin plate of bone or silver is introduced beneath the eyelid, and the border then cut off. The knife used by Jüngken in this operation is represented in fig. 47.
2. Of Cataract. By this is understood an opacity of the crystalline lens or its capsule by which vision is obstructed either totally or partially. When the lens alone is affected, the cataract is lenticular; when the capsule alone, capsular; and capsulo-lenticular when both are concerned.
In operating for cataract, the lower eyelid is to be drawn downwards and outwards by the index and middle finger of the left hand of the operator, while an assistant supports the chin with his left hand and holds back the upper eyelid with his right.
All the different operations for cataract have as their object the displacement of the lens and capsule. This is effected either by removal through the cornea or sclerotic, by pushing to one side, or by cutting into pieces so as to cause the absorption of the fragments.
a. Extraction. This operation involves three stages: 1, the opening of the eyeball by means of semilunar incisions in the cornea; 2, the opening of the capsule; and 3, the removal of the lens through the pupil. The incision is made with the cornea knife, the form of which varies greatly (pl. 140, fig. 59, Beer’s knife; fig. 57, Bell’s knife; fig. 58, Sharp’s knife). The right eye must be operated with the left hand, the left with the right (pl. 139, fig. 10, operator with Beer’s knife; fig. 11, do. with the double knife of Jäger). Jäger’s knife is asserted to have the advantage of causing a wound which heals sooner, and without as much probability of the protrusion of the iris and vitreous humor. A modification of Jäger’s knife (pl. 140, fig. 61) has been proposed by Ott. After the incision has been made through a little more than one half of the circumference of the cornea almost close to the sclerotic, the upper eyelid is to be dropped for a few seconds, and then carefully raised for the introduction of the instrument intended to open the capsule. This is best effected by the lancet-shaped cataract needle. Instruments called cystitomes (fig. 60, La Faye’s as improved by Richter) have been recommended by some, but they are liable to serious objections. Three or four vertical and several transverse scratches of the capsule are now made with the cataract needle. The lens will then usually come out of the capsule, but may require the assistance of a gentle pressure. Various attempts have been made to extract the capsule with the lens, and for this purpose different forceps have been invented, such as Beer’s forceps, (fig. 44), Graefe’s do. (fig. 45), Maunoir’s do. (fig. 46). The experiment of making the entrance through the sclerotic has been attended with considerable difficulties and dangers, so that the present method is most generally employed, excepting where the next mentioned is preferred.
b. Keratonyxis consists in the introduction of a needle through the cornea for the purpose of breaking up the cataract, separating it from its connexions, in order that it may be dissolved and absorbed; or else to depress it and thus force it out of the axis of vision. The latter operation is more correctly termed couching.
Both curved and straight needles may be used in these operations; the former, however, are preferred. The operator pierces the lower part of the cornea, far enough from its border to clear the pupillary margin of the iris (pl. 139, fig. 12).
Bowen has proposed a mode of operating which, he calls hyalonyxis (fig. 13); a curved needle, with the convexity anterior, is so introduced, about three or three and a half lines from the margin of the cornea, and one line beneath the transverse diameter, as to enter the vitreous hrynor behind the lens and capsule; the posterior wall of the capsule is torn, the lens depressed in the vitreous humor, and the anterior wall of the capsule then torn in a similar manner.
3. Contraction and Obliteration of the Pupil (Syninesis, Obturatio, Imperforatio, Phthisis pupillæ, Atresia iridis). There are three methods by means of which an artificial pupil can be obtained: 1. By cutting the fibres of the iris (coretomia or iridotomia); 2. By cutting out a segment of the iris (corectomia, iridectomia); 3. By destroying the connexion between iris and ciliary ligament (coredialysis, iridodialysis). Sometimes two methods are combined, for the sake of greater certainty.
In iridotomy and iridectomy, an incision is first made in the cornea, through which the operator introduces a pair of very delicate scissors (pl. 140, figs. 42, 43), which may be either straight or curved; these are to be opened, and one point to be inserted into the iris, and a section made running towards the transverse diameter. A second section is so made as to include a V-shaped piece between the two (pl. 139, fig. 14). Owing to the not unfrequent junction of the iris at the edges of the insections, the second mode of operation was resorted to, that of iridectomy, in which a pupil was formed by cutting out a portion of the iris. This is conducted in a manner similar to the last processes; the piece there formed is taken up by fine forceps (pl. 140, figs. 44, 45, 46), and cut off with fine scissors. The hook-forceps (fig. 44) have been used to advantage in these and similar operations, to insure a firm hold of the object to be grasped.
Hare-Lip
Hare-lip is a congenital malformation of the lip, an arrest in the development of it while the remaining portions of the system have advanced to proper perfection. It generally occurs alone, but frequently is found associated with a fissure of the palate.
The first part of the operation consists in paring the edges of the lip, either with scissors or w4th the scalpel.
In operating with the scissors (pl. 139, fig. 17), the lower corner of the fissure is grasped with the hand or a hook, the lip drawn downwards and outwards, the blunt edge of a tolerably strong pair of scissors is introduced between the jaw and the lip, and the borders of the incision are taken off at a single cut. The bent scissors represented in pl. 140, fig. 18, are most convenient for this purpose. After the cuts have been made on each side of the fissure, the second stage of the operation is to be carried out, consisting in the approximation of the wounded edges, which are retained by needles, but sometimes by adhesive plaster.
The bloody suture (sutura cruenta) is effected in various ways. The figure-of-eight suture is the one most usually employed, and for this reason frequently called hare-lip suture. The shape and size of the needles vary greatly. Dieffenbach made use of fine insect needles or pins, which, after being properly wrapped, are cut off close to the thread. Two needles usually suffice for children, three for adults. Pl. 139, fig. 18, a b c, shows the mode of introducing the needles. As soon as a needle is inserted, it is wrapped with thread and fastened, and a common thread may finally be wound over all the needles (fig. 19). Should the lip be much drawn up or shortened, circular incisions may be made on each side, as shown in fig. 20, a b.
Cleft Palate
A fissure of the palate is frequently found associated with hare-lip: it may be a congenital disease, or the result of injuries or diseases of after-life. Like hare-lip, too, it is an arrest of development which prevents the corresponding lateral portion of the palate from uniting along the median line to form a continuous roof to the mouth.
Formerly it was the custom in such cases to supply an artificial roof to the mouth by means of a plate of gold, silver, horn, &;c. This answered more or less satisfactorily for fissures of the hard or bony palate, while fissures of the soft palate were, until quite recently, considered irremediable and incurable. The operation of suture of the palate, better known as staphyloraphia, was first attempted by Græfe in 1816. This consisted in paring off the edges of the fissure, which were afterwards brought into such approximation that the sides united perfectly. Experience, too, has shown that the operation not only obliterates the fissure in the soft palate, but ultimately that in the hard palate likewise.
A piece of cork is required to be placed between the back teeth, for the purpose of keeping the mouth open during the operation. Different kinds of knives have been made use of to pare the edge of the fissure, as also various forceps and tenacula for arranging the edges. Ligatures of about two feet in length are necessary. Various forms of needles, needle-holders, and forceps are required for making the attachment, and special instruments are required for tying the knots.
The operation is conducted as follows: The mouth of the patient is opened, and the base of the tongue depressed. With a knife, having a blade somewhat like the edge of a lancet, the cutting edge about a quarter of an inch in extent, and the flat surface bent semicircularly. an incision is made about half an inch long on each side of the posterior nares, a little above and parallel to the palatine flaps, and across a line straight downwards from the lower opening of the Eustachian tube, by which the levator palati is divided on both sides, just above its attachment to the palate. The edges of the fissure are next pared with a straight blunt-pointed bistoury, removing little more than the mucous membrane; then, with a pair of long, blunt-pointed, curved scissors, the posterior pillars of the fauces are divided just behind the tonsil, and, if necessary, the anterior pillar likewise; the wound in each part being about a quarter of an inch in extent. Lastly, stitches are introduced by means of a curved needle set in a handle, and the threads tied, so as to keep the edges accurately in contact (pl. 139, fig. 31).
Odontalgia
Diseases of the teeth are so numerous and important, that their treatment constitutes a separate branch of surgery. We shall here only refer briefly to the principal instruments used in the extraction of teeth, usually the only method by which odontalgia, or tooth-ache, can be effectually cured. In the multiplicity of contrivances for extracting teeth under all possible circumstances, we can find room for comparatively few.
The first step in the extraction of teeth consists in cutting the gum around the neck of the one affected. Convenient instruments for this purpose are those invented by Cruce (pl. 140, figs. 69, 70). They consist of two handles with sharp bent extremities. Pare’s apparatus (fig. 71) is a steel rod, fastened into a handle, and with a spatulate bent end.
For the extraction, we have first the parrot-healced forceps (fig. 72), with a spring between the handles to keep them apart. Fig. 73 represents the large curved forceps for extracting canine and anterior molar teeth. Mortet’s forceps (figs. 74, 75).
Pl. 139, fig. 28, illustrates the mode of extracting a lower incisor by means of the forceps.
The simple key (pl. 140, fig. 76 a b) consists of a steel stem, four and a half inches long, with a wooden or bone handle. Into an incision in the bent upper end, the hook, b, is inserted and retained by a screw.
The key with movable hooks (fig. 77) is much like the preceding, except in having an offset, a, which receives the hook, b, and is held by a screw.
Pl. 139, fig. 29, exhibits the method of extracting a back tooth by means of a key. The stem of the instrument is usually wrapped with a handkerchief, to prevent contusion of the gums.
Restoration of Lost Parts (Chirurgia curtorum, Transplantatio, Merioplastice)
This art has been known for a long period of time. It depends upon the highly interesting physiological phenomenon, that parts of the body maybe separated and transferred to another part, or even to an entirely different individual, and yet form a vital and persistent attachment. It is in cases of deficiency or malformation of parts of the face, that this art has been made use of with greatest success, and especially in the formation of a new nose, known as the Taliacotian or rhinoplastic operation.
Restoration of the nose by means of a flap from the forehead. In the first place, a model corresponding to the face and stump of the nose is to be constructed of wax or clay; this measured with strips of paper, and the outlines thus obtained marked off on paper and cut out. This outline is then to be spread out fiat on the forehead, the base uppermost, the apex at the top of the nose, and marked out on the forehead with ink. Dots of ink should also indicate where the sutures are to be made, four on each side being usually sufficient. The operation itself presents four stages. In the first, the margin of the outline on the forehead is to be cut through, excepting the narrow neck between the eyes, and the flap of skin dissected from the periosteum. When the bleeding has ceased, the flap is to be twisted on itself, and its edges fitted into the grooves made for its reception, and these fastened with sutures. A roll of oiled lint is then to be introduced into each nostril, for the purpose of supporting the nose, and a pledget above the septum; the wound on the forehead filled with dry lint; and the ligatures removed after from forty-eight to seventy-two hours. After adhesion has thoroughly taken place, the twisted strip of skin by which the connexion with the forehead was maintained, is to be cut through, or a little strip cut out, so that it may be laid down smoothly. (Pl. 139, fig. 21.)
This mode of operating has experienced various modifications by different surgeons. Pl. 139, fig. 24, represents the method adopted by Delpech in a particular case; fig. 25 is the flap of skin brought down and then twisted.
Fig. 22 exhibits a newly formed nose, after Dieffenbach, in which all the hard parts had been lost, and the soft parts either destroyed by suppuration, or fallen in. The soft parts were first trimmed off even, and dissected out to a slight amount beneath the skin of the cheeks, and a transverse incision made in the upper lip to receive the septum; after this the flap was brought down from the forehead and attached as before described. Some surgeons prefer to form the septum of the nose by a subsequent operation from the upper lip.
When the nose is to be formed out of the skin of the arm, a model of it is to be made, and the surface of the model cut out in paper and marked off on the arm. Groefe has invented a special apparatus for connecting the arm and face, consisting of a cap, jacket, and arm bandage, shown in pl. 139, fig. 26. The cap, a, is prolonged on each side in a flap, c, by means of which it is fastened under the chin. Above is sewed to it the bandage, d, for holding the wrist. Opposite threads are attached to the cap, which are tied together to hold the bandages, p, q, r; two are at g, two at c, and two on the other side of the head opposite to g. A small ring is fastened at f with strong tape, and through it passed a bandage, by which the entire head may be drawn back towards k, if necessary. The cap is attached to the jacket, b, at u. A second ring is placed at i for the purpose, by means of a tape, of drawing the arm towards the left, if required; another is situated on the right side. The pantaloons are fastened to the waistband, h. The arm bandage consists of the linen band, l, m, n, o, with six side bands; the former consists of a part for the upper arm, s, n, and the forearm, s, l. The arm portion is attached along the border, m, o, to the three side bands, p, q, r, by nine narrow tapes or silk strings; the same arrangement exists on the opposite side. The position of the side bands is secured by the six strings attached to the cap.
Fig. 27 represents the flap of skin dissected from the arm and attached to it only by its base. It is cicatrized along its margin and under surface, and thereby prepared for attachment to the stump of the nose.
Extirpation of portions of the Tongue
For this operation will be needed a piece of cork, and a polypus forceps, or Muzeux’ tenaculum forceps (pl. 140, fig. 12). It will sometimes be necessary to pass a string or loop through the sound part of the tongue, for the purpose of drawing it out during the operation, and for stopping the flow of blood. There will also be required a straight, a sharp, and a blunt bistoury, a Cooper’s scissors, ligature apparatus, cautery irons, cold water, ice, &c. The tongue of the patient is to be protruded as far as possible, and held by forceps or a loop. The operation itself is conducted either by means of an incision or by ligature.
Pl. 139, fig. 30: at the points g and h, two needles are passed through from beneath, each provided with a separate and a common thread, the latter of which, g, k, h, i, is tied on the back of the tongue; the two former, g, l, m, and h, n, o, are fastened in the edges. For removing the small portion of the side of the tongue, a needle with a double thread is passed through at p, and the two ends of those tied together at q and r.
Œsophagotomy
This is resorted to sometimes for the removal of foreign bodies, partly for the purpose of introducing, food.
For the first end, three methods have been proposed, that of Eckholdt with the most favor. The operation is to be performed in the triangular space included between the two crura of the sterno-cleido-mastoid and the clavicle. The skin is in an obliquely transverse fold, and an incision made of about two inches in length, running downwards and inwards to the sternal end of the clavicle, and the platysma separated. Should the space between the muscular portion be too much confined to permit a sight of the laryngeal nerve lying along the œsophagus, the angle of the two heads is opened up on a director by introducing this close behind the muscle, and thus avoiding any danger of injuring the inferior thyroid artery and the omo-hyoid muscle. The omo-hyoid may be then pushed up, the carotid artery and jugular vein outwards, the œsophagus laid bare, and then opened either against the foreign body or a small aperture made and enlarged with forceps, or by the introduction of a director.
Pl. 139, fig. 32, the lips of the incision are separated by means of two double tenacula: 1, sternal, 2, clavicular portion of the sterno-cleido-mastoid muscle; 3, stern o-thyroid muscle; 4, omo-hyroid do.; 5, thyroid gland, 6, trachea; 7, carotid artery; 8, inferior thyroid artery; 9, laryngeal nerve and branches; 10, cellular tissue.
To extract the foreign body after the operation, we may make use of a straight forceps (pl. 140, fig. 15), or if it be some distance from the opening, of a curved forceps as shown in fig. 78. Degenerate portions of the membrane of the œsophagus, false membranes, &c., may be removed with the knife or with the scissors. The introduction of nourishment when necessary is to be effected by means of a flexible tube.
If the foreign body be not too large it may in most instances be removed without an operation. An instrument for extracting such substances, invented by Petit, and improved by Eckholdt, is shown in fig. 79. It consists of a handle, a; a ferule, b; a whalebone rod, c c; a silver tube with two hooks, d, to which is fastened an elastic tube, e e; f is a long cylindrical piece of sponge to which are attached some loops of thread, g, to catch hold of small angular bodies.
For the extraction of bodies of moderate size Eckholdt made use of the apparatus shown in fig. 80. An elastic catheter, g g, is provided at its superior extremity with an open convex silver ferule attached to it by two arms. Into the catheter is passed a round whalebone rod with a wooden handle, which carries a silver ferule, b. This ferule, c, has a ridge, c, round its margin, cut through in two opposite places; a silver tube, e, on the catheter has a small hook, f, on each side, which passing through the breaks in the ridge, e, and slightly rotated, serves to unite the catheter to the handle. The whalebone rod projects about two inches beyond the tube, and to its anterior end is fastened a small silver button having eight grooves radiating from the centre, cut on its surface. In these are laid four thin whalebone rods about five inches long, and crossing each other in the centre of the button; these are held in place by a small cap with eight teeth, which bend down between the rods and thus keep them in place; they are then bent over and tied along the anterior end of the tube, and afterwards surrounded by a ferule with the anterior margin bent in between the rods to keep them at a proper distance apart. The cage thus formed will of course be enlarged and expanded on drawing back the rod, and on the other hand elongated and greatly diminished in diameter by pushing the rod out or forwards. To extract pins or other sharp bodies, the cage may be covered with a small bag of fine silk, and also encircled by numerous loops of thread.
Amputation
Amputation proper has reference to the cutting through of a limb: when the separation takes place at a joint, we have excision, or ex-articulation.
Amputating apparatus consists of the following instruments: two tourniquets (pl. 140, figs. 86–88, those of Henkel and Savigny); amputating knives of various sizes, single edged for circular sections, and double edged for flap operations (fig. 84, Savigny’s knife; fig. 85, Weiss’s knife for circular incision); a straight or bellied bistoury; knives for separating bone and cutting periosteum; amputating saws (fig. 21, Pott’s saw); bone nippers for extracting spicula (fig. 20); bone scissors (fig. 19) and rasps; a chisel (figs. 22, 23); forceps (figs. 35, 36); artery tenaculum (fig. 37, Bell’s); and the necessary bandages. Good assistants, generally five in number, will be required. The suggestion of Moore, to diminish the pain of an operation by compressing the principal nerves (fig. 89, nerve compressor), has not been much followed.
Various tables have been constructed for the suitable arrangement of the patient (fig. 90, Kluge’s table), but these are only applicable in hospitals.
The principal modes of amputation, subject, however, to numerous modifications for the different regions, are two in number.
1. The Circular Method. This may be either simple or double. In the simple incision, all the soft parts are cut to the bone, then pushed up, and the bone sawed off close to the muscle. Subsequently it was considered preferable to cut first through the skin, then pushing this up to cut through the muscle, and finally to separate the bone as before.
2. Flap Operation. The flesh is grasped by the surgeon, and lifted from the bone; the double edged knife is passed horizontally through it, the point carried over the bone, and pushed through the other side of the limb; it is then made to cut its way out upwards and forwards, so as to make the anterior flap. The knife is again entered on the inner side a little below the top of the incision, passed behind the bone, brought out at the wound on the outside, and directed so as to make a posterior flap. Both flaps are now drawn back, the knife swept around the bone to divide any remaining muscular fibres, and the bone sawed through.
Pl. 139, fig. 33, amputation of the thigh: a, b, hands of the first assistant; c, d, do. of second assistant; e, f, operator.
The following figures are intended to illustrate the respective positions of the individual parts after an amputation.
Pl. 139, fig. 34, circular amputation of the upper arm, three and a half inches above the middle: a, humerus; b, c, deltoid muscle; d, long, e, short head of the biceps brachii; f, latissimus dorsi muscle; g, h, i, k, l, triceps brachii; m, n, o, p, subcutaneous adipose and cellular tissue: 1, brachial artery; 2, posterior circumflex artery; 3, basilic vein; 4, 5, deep seated brachial vein; 6, cephahc vein; 7, median nerve; 8, ulnar nerve; 9, middle cutaneous nerve. Fig. 35, circular amputation of the thigh two inches below Poupart’s ligament: a, femur; b, rectus femoris; c, sartorius; d, vastus externus and tensor vaginæ femoris; e, vastus internus; f, adductor longus; g, gracilis; h, i, k, l, adductor magnus, adductor brevis, and semi-membranosus muscles; m, biceps cruræus; n, semi-tendinosus; o, adipose and cellular tissue between the adductors and gracilis; p, q, r, t, subcutaneous adipose and cellular tissue; s, intermuscular tissue; 1, cruræal artery; 2, deep do.; 3, external circumflex artery; 4, cruræal vein; 5, 6, 7, deep seated veins; 8, saphena major vein; 9–22, small and large muscular and cutaneous arterial branches; 23–25, branches of the cruraeal nerve.
Fractures
These occur in all the individual bones, although more rarely in some than in others.
In treating fractures, a point especially to be attended to is the transportation of the patient, especially if the distance be considerable. In the treatment proper, the first step consists in properly approximating the fractured extremities, and then in keeping them undisturbed in close contact; the rest must be left mainly to the recuperative energies of the system. Pl. 140, fig. 91, represents a bed well adapted for the ease and immobility of the patient while under treatment for the union of a broken limb.
Calculus
Calculus, or stone in the bladder, is a very painful disease of frequent occurrence. Owing to the danger of a direct operation for this disease, efforts have frequently been made to discover methods by means of which such operation might be avoided. The great objection to these methods, known under the general name of lithontripsy, is, that they do not act directly upon the calculus, and that their long continued use, which is usually necessary, introduces a train of new evils.
We cannot pretend to enter into even a brief account of the various methods of performing operations of lithotomy, or extracting the calculus directly, as this would of itself require a volume. We must confine ourselves to a reference to some forms of apparatus, by which the stone may frequently be broken up in the bladder and evacuated in minute fragments. The instrument invented by Civiale, and called lithotriptor, has been made use of with considerable success, although liable to the danger of lacerating the coats of the bladder, and of bruising the parts about the neck. It is represented in pl. 140, figs. 81–83, and consists essentially of a straight cylindrical canula introduced into the bladder, and containing three or four branches which can be protruded by external machinery These are then made to grasp the stone and hold it tightly, whilst it is bored, scooped, and excavated by drills contained in the centre and worked by a bow. When the stone is sufficiently excavated, its shell is crushed into small pieces.
The instrument most used at the present day is the screw lithotrite, composed of two sliding blades, between which the stone is seized and crushed by gradual pressure with a screw.